どうも、CBDを愛してやまないCBDハッカーだ。
このページでは、100種以上のCBDを経験してきた私が心からおすすめできるリキッドを紹介したい。
またありきたりな量産ランキングページではなく、より良いCBD製品を使って欲しいという一心から、私なりに出来るだけ分かりやすく書かせていただいた。
そのため「当たりのCBDが欲しいな・・初めてだから失敗しないリキッドを使いたいなぁ」と思っている方には、ぜひ読んでいただきたい内容である。
なお、本記事の構成は下記のとおりだ。
さて、前置きはこれくらいで。
早速見ていこう。
CBDリキッドの選び方
まずは、選び方の基準を紹介したい。
①:CBDの濃度
②:フレーバー
③:CBDの種類
この3点を理解すれば自分の好みに限りなく近いリキッドを選べるため、サクッとでいいので読み進めて欲しい。
その①:CBDの濃度
リキッドには、CBDがどれだけ含まれているかを示す「濃度」がある。
そして結論として、初心者なら「5%」もしくは「10%」の濃度が良い。
なぜならCBD感をきちんと体感でき、かつ「1番吸いやすい濃度」であるからだ。
5%より低濃度の場合だと、人によっては何も感じないことがあり、逆に10%より高濃度の場合だと、激しくむせることがある。
だからこそ、「5%」か「10%」を選ぶべきということを理解しておくべきだ。
その②:フレーバー
フレーバー選びも重要だ。
同じ商品でも、10種ほどのフレーバーを用意しているメーカーもある。
なので本記事のランキングでは、「どのフレーバーが吸いやすかったか」という点も細かく書いていく。
その③:CBDの種類
CBDには、大まかに下記の2種類が存在する。
・単一CBD
・フルスペクトラムCBD
単一CBDとは、その名の通りCBDのみが含まれた製品だ。
そしてフルスペクトラムCBDとは、CBD以外にもCBGやCBNなどの成分が入っている製品のことである。
なおCBDは、CBGなどの他の成分があることで、より効果が高まることが分かっているのだ。
つまりまとめると
①:5%~10%のリキッドを探す
②:好みのフレーバーがあるか確認
③:フルスペクトラム型ならラッキー
あなたが初めてCBDリキッドを使うなら、上記が「1番失敗しないリキッドの選び方」だ。
なおフルスペクトラム型製品は数少ないため、好みのリキッドがフルスペ仕様ならガッツポーズをしておきたいところ。それくらい、満足度は桁違いに違うのだ。
CBDリキッド|総合おすすめランキング10選
さて、ここからが本記事のメインだ。
「これなら間違いない、失敗しない」と断言できるCBDリキッドを10個紹介する。
なお先に書いておくと、初心者の方には上位3つのどれかがおすすめである。
それだけ、口コミ評価も高いリキッドなのだ。
おすすめ1位 PharmaHemp(ファーマヘンプ)

| 濃度 | 容量 | 種類 | 価格 |
| 5% | 10ml | フルスペ | 8,900円 |
ファーマヘンプが、文句なしの1位だ。
こちらはヨーロッパのスロベニア産CBDを採用しており、質が高いことからかれこれ3年以上は圧倒的な人気を維持している製品である。(ヨーロッパでは古くからCBD栽培が行われており、製品としての質が高いことで有名。)
そして濃度は5%で、かつフルスペクトラム型だ。そのためCBD単一の製品よりもしっかりとしたキック感があり、満足度はかなり高い一品だと思う。またむせるほどのキツい吸いごたえはないため、初心者の方にはピッタリなはずだ。ちなみにリキッドの色合いは下記のとおり。

つまり「むせることはなく、CBD感をしっかりと味わえること」がファーマヘンプの魅力だ。
またフレーバーも10種用意されている。
・ライム
・カンナビス
・ティラミス
・ピニャコラーダ
・グリーンアップル
・メンソールブルー
・バニラカスタード
・ハネデューメロン
・アマレーナチェリー
・クリーミーストロベリー
この中でも特に、「ライム」「ティラミス」「メンソールブルー」が中毒的な美味しさを感じた。
決め付けるようで申し訳ないが、初めてのCBDリキッドにはファーマヘンプの一択しかないと思う。おそらく、このレベルの製品で不満を覚える方はいないだろう。
1つ目は、「初心者キット」の存在だ。

上記の初心者キット(9,700円)では、リキッドの使用に必要なバッテリーとアトマイザーがセットで買える。
単品で購入するよりも2,000円ほど安く購入できるため、まだ手元に何も無い方には必見のセットだ。
2つ目は、20%引きクーポンについて。
当サイトから、販売サイトである「CBDMANiA」にアクセスし、「CBDMANiA20」のコードを入力すると、20%引きで購入できるのだ。つまり初心者キットなら、「9,700円→7,760円」といった具合である。
7,000円台は高く感じるかもしれないが、このプレミアムブラックシリーズのリキッドは最高にたまらない製品だ。
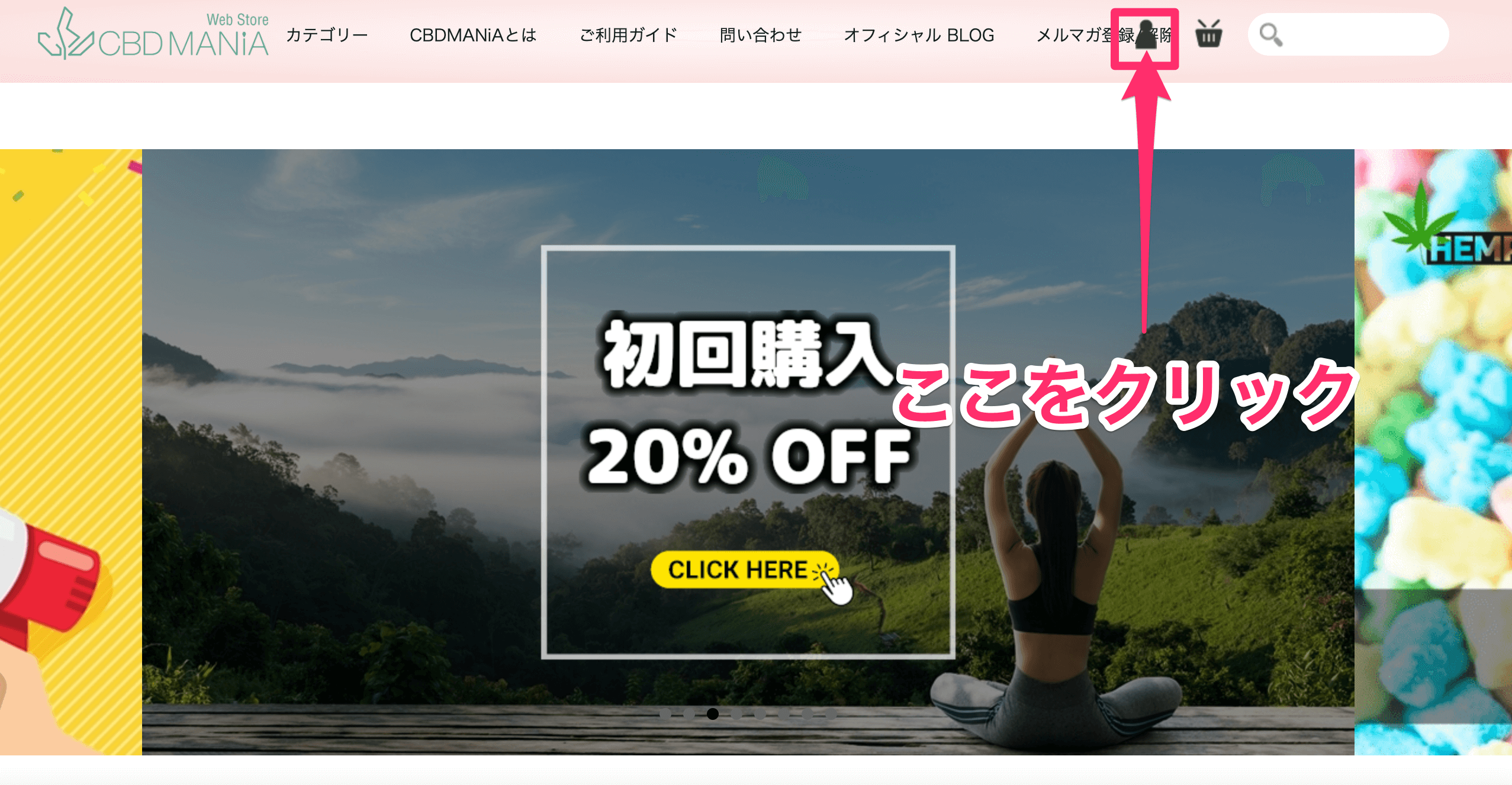

単品で購入する場合でも操作は同じだ。
まず商品ページに移動し、フレーバーとカラーを選択する。
そして、「カートに入れる」をクリックしよう。
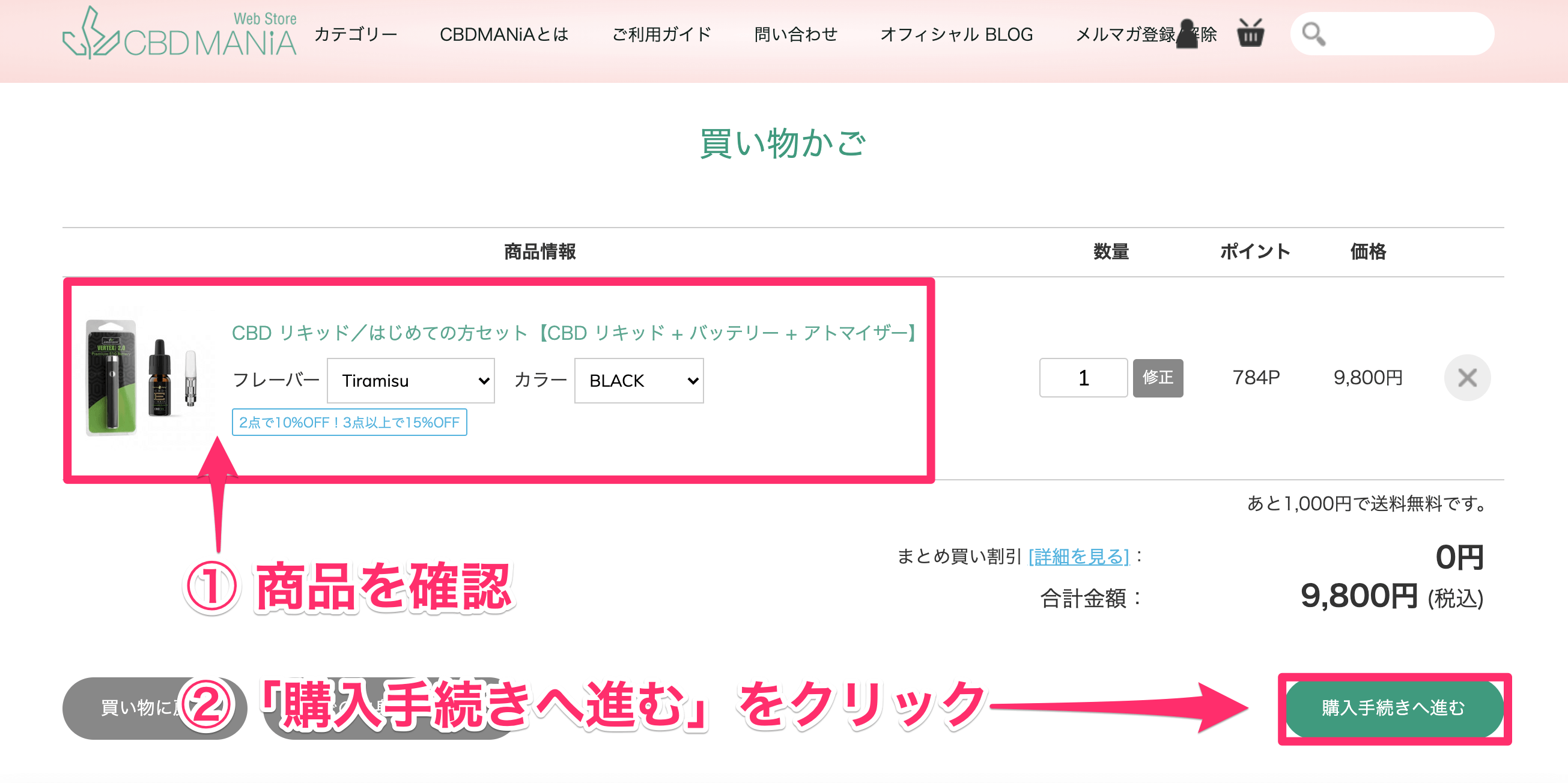
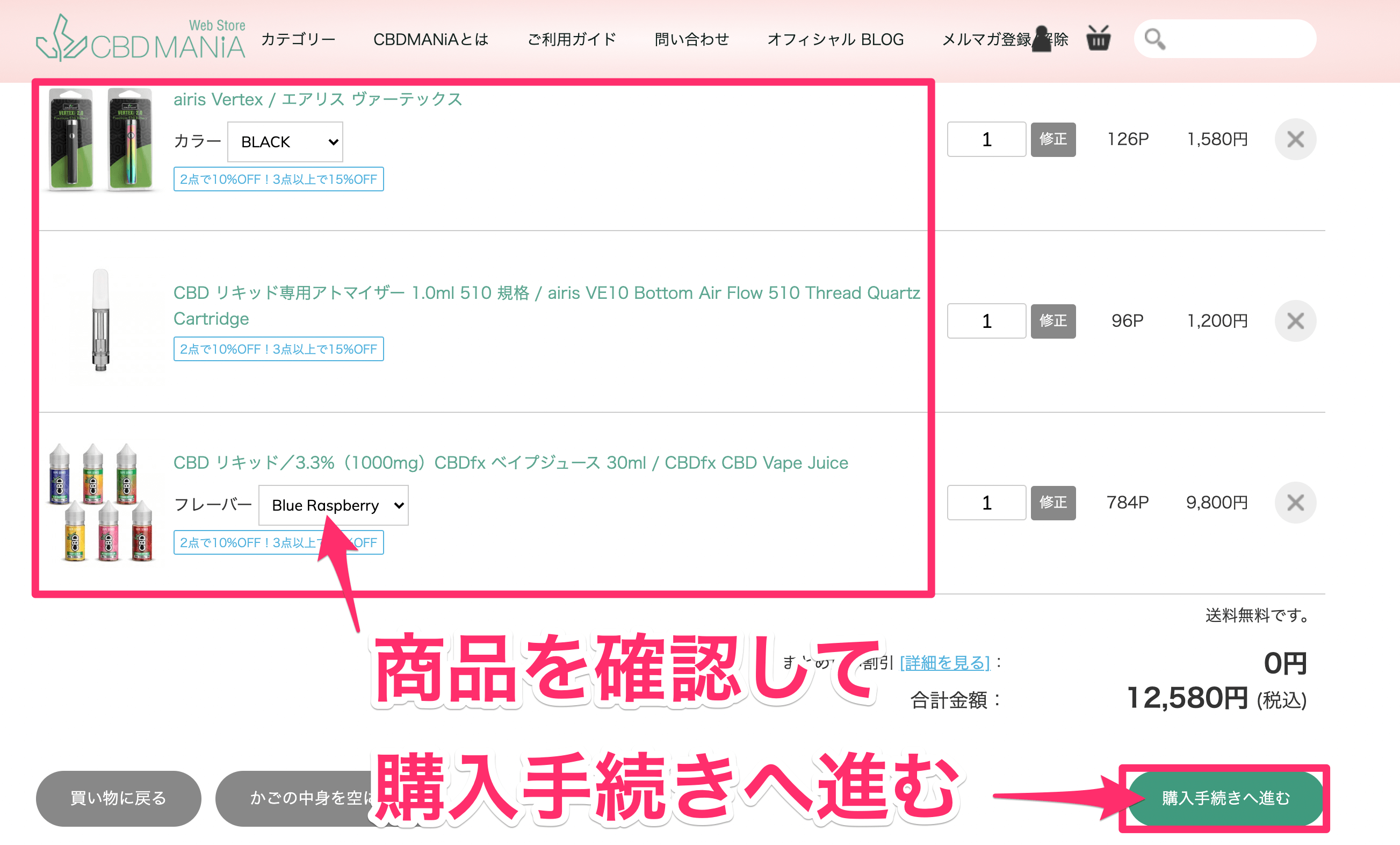
購入する商品が正しいことを確認する。
そして、「購入手続きへ進む」をクリックしよう。
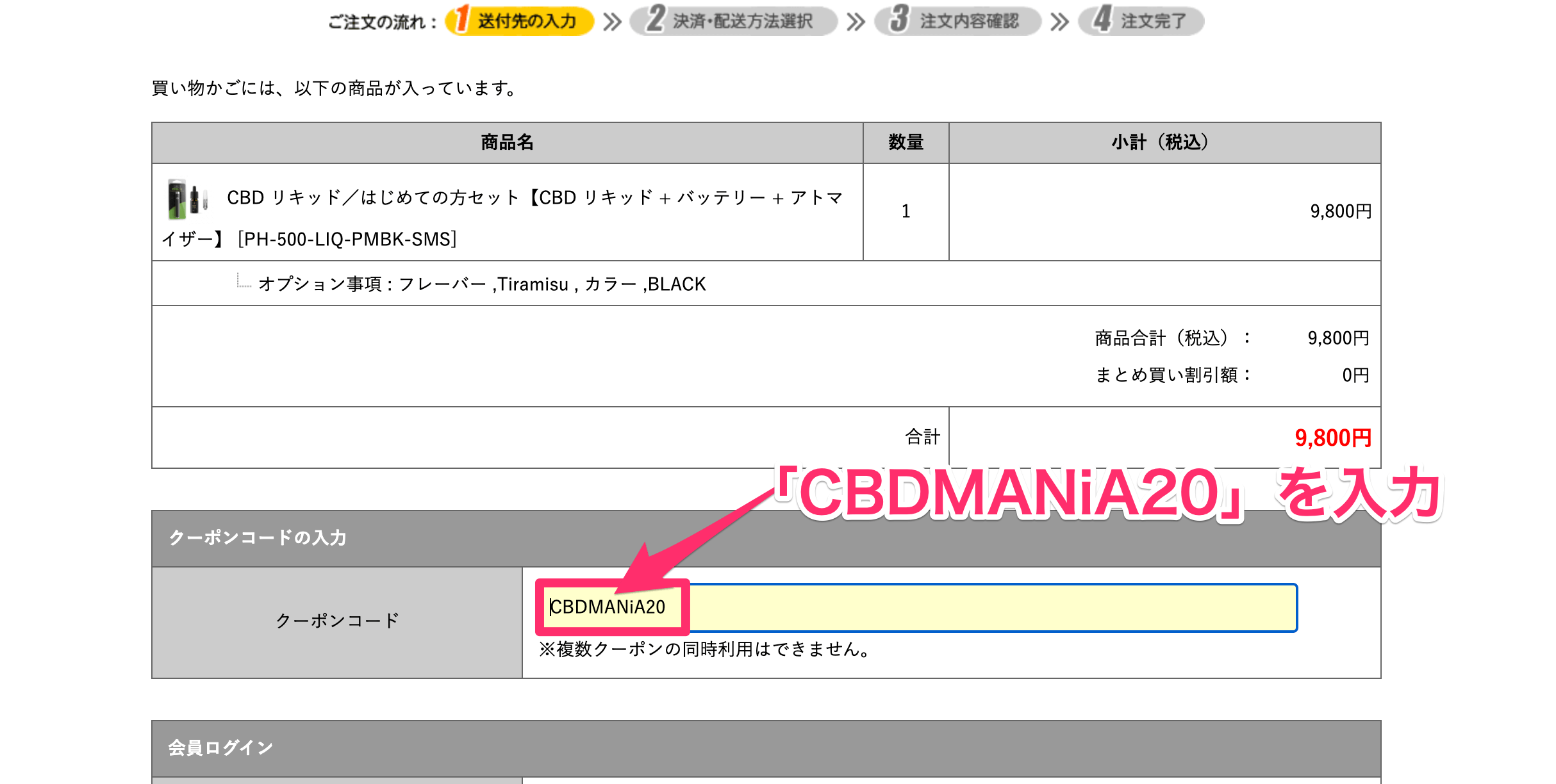
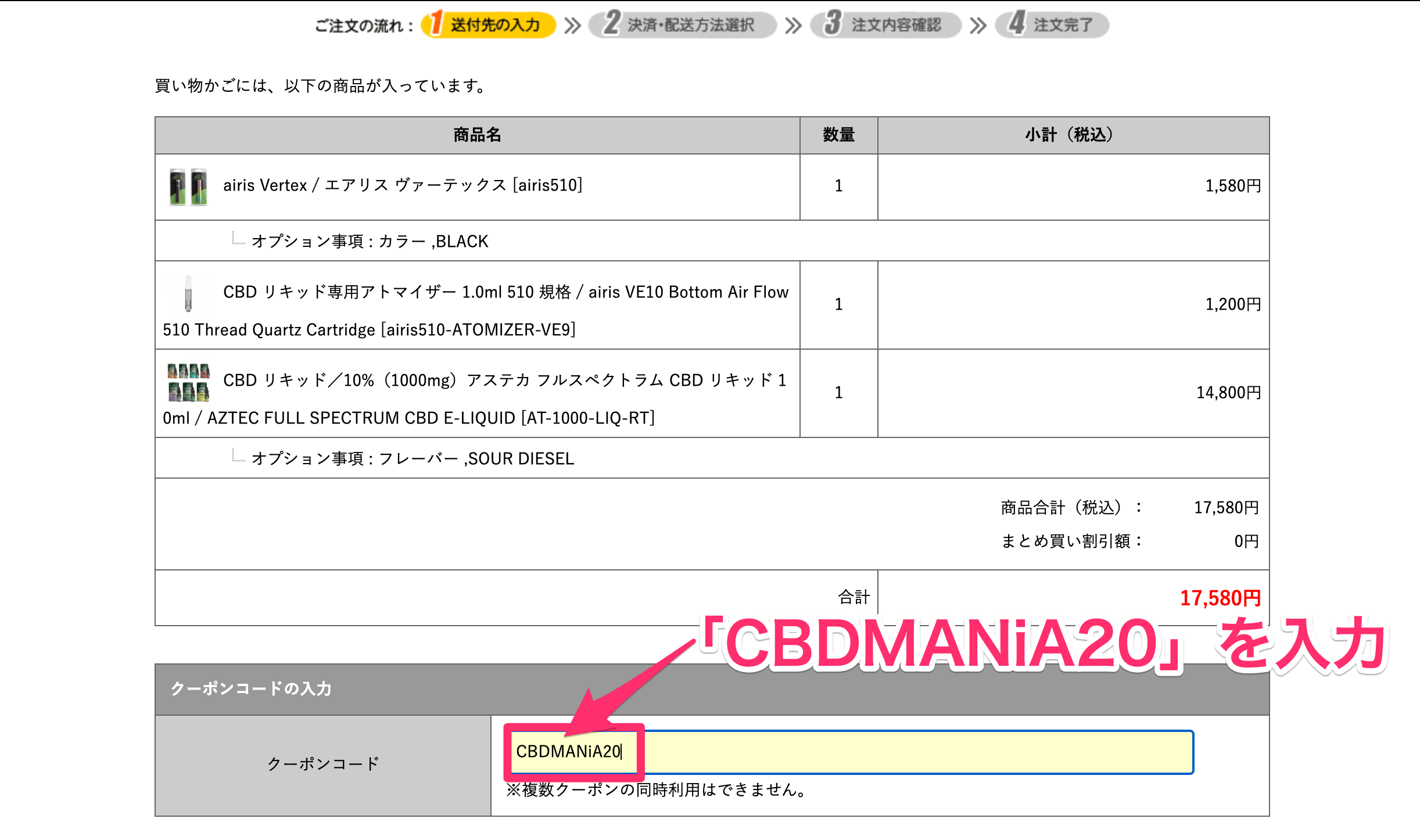
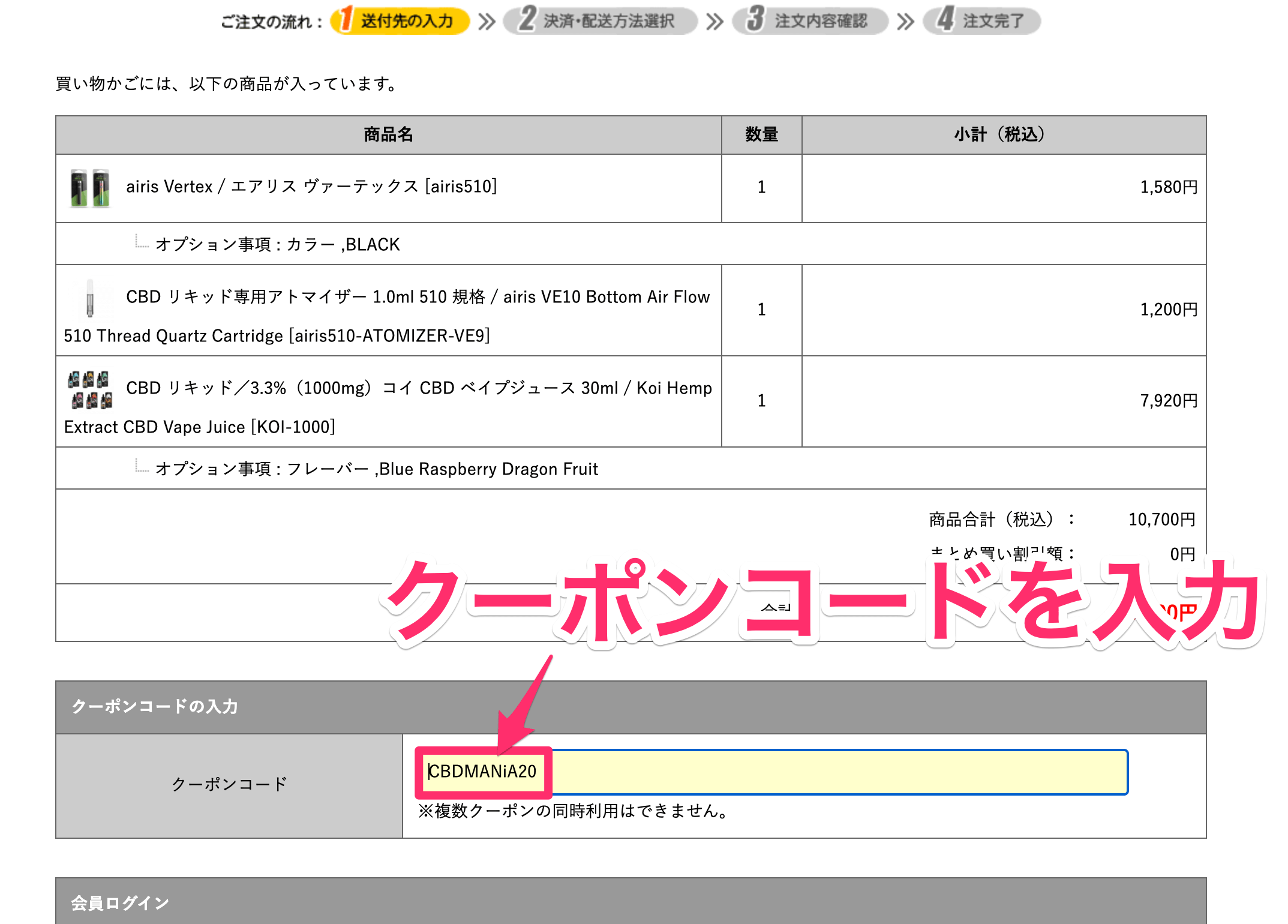
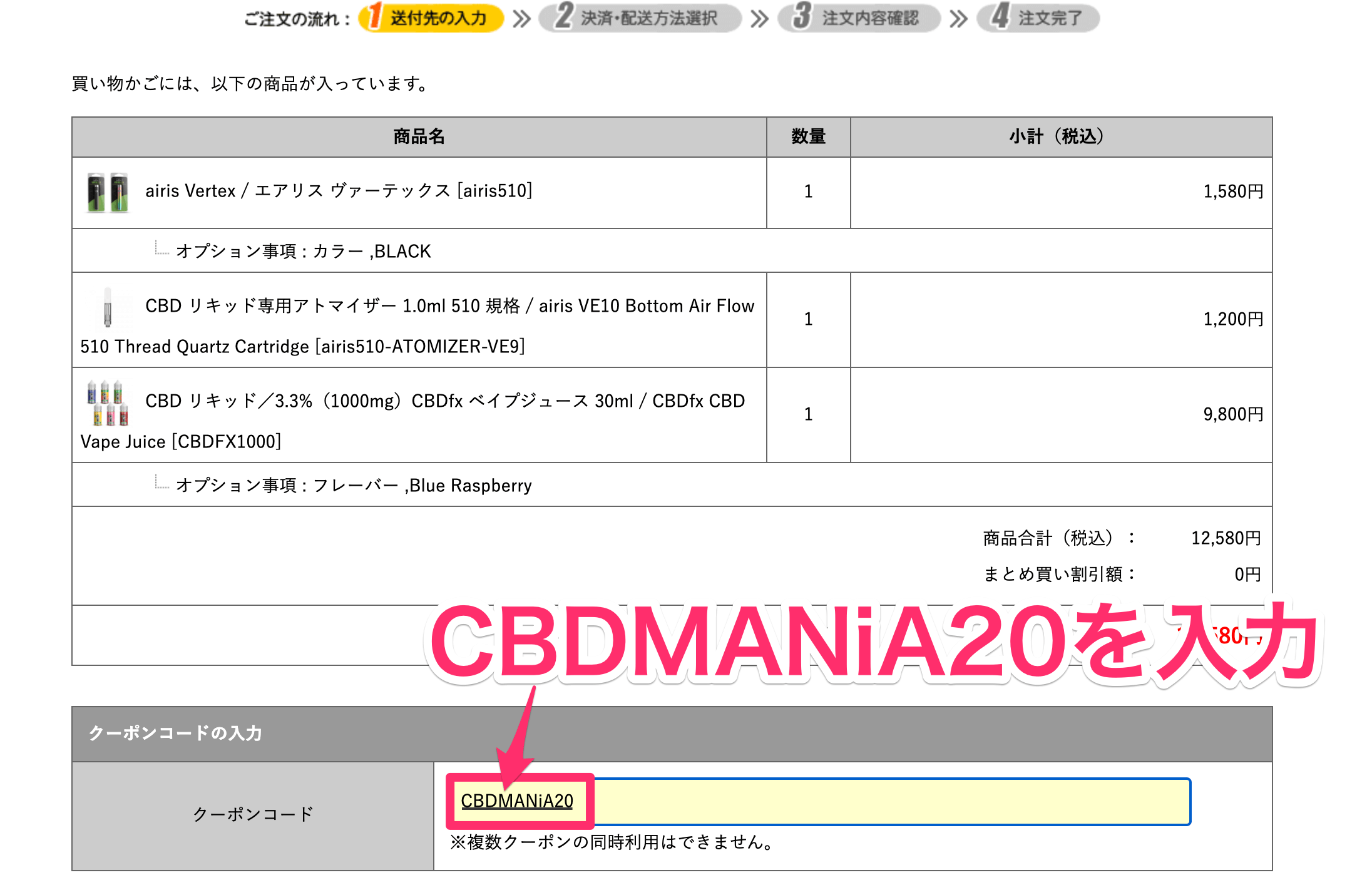
ここで、「CBDMANiA20」を入力する。
入力すれば、20%引きが適用される仕組みだ。
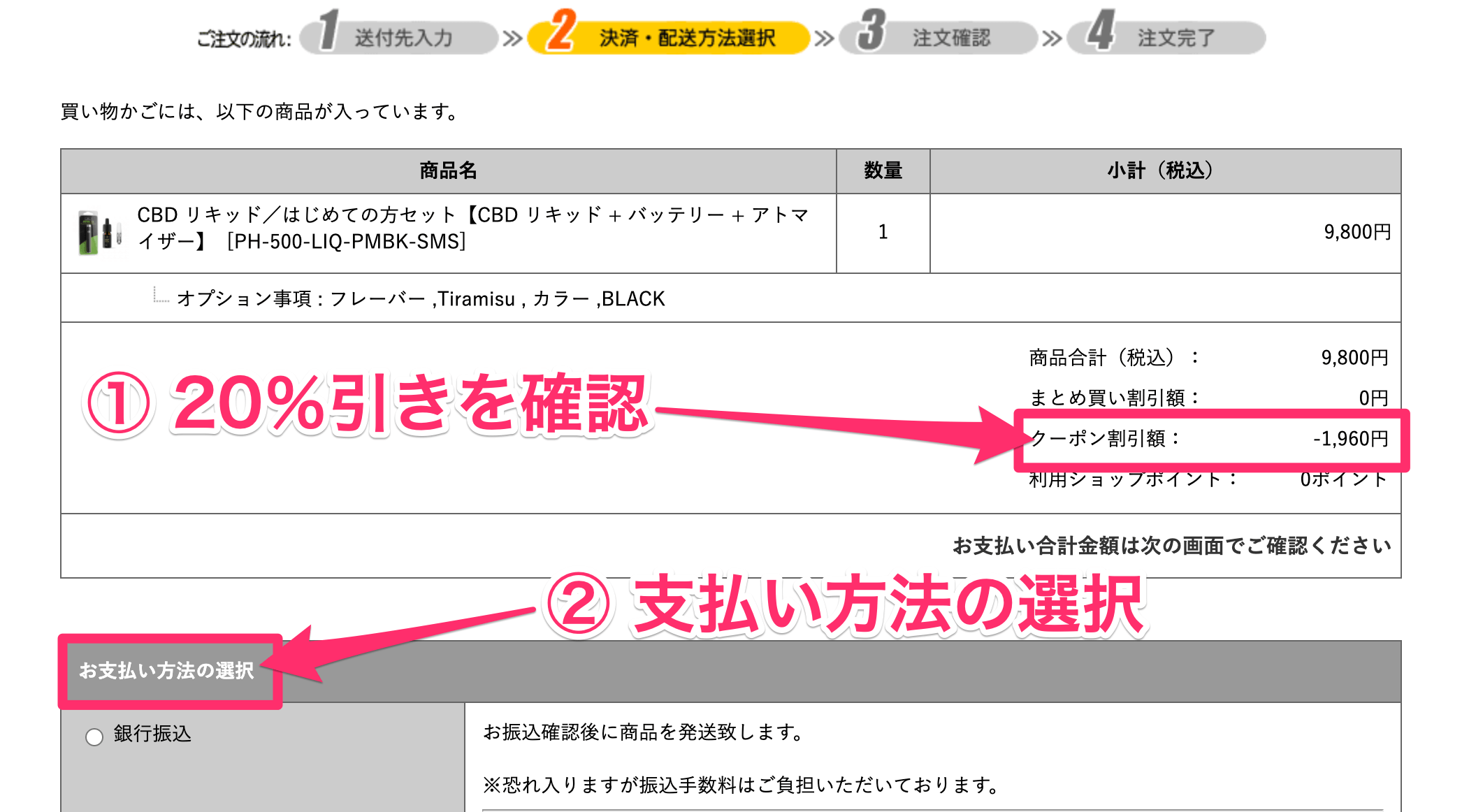
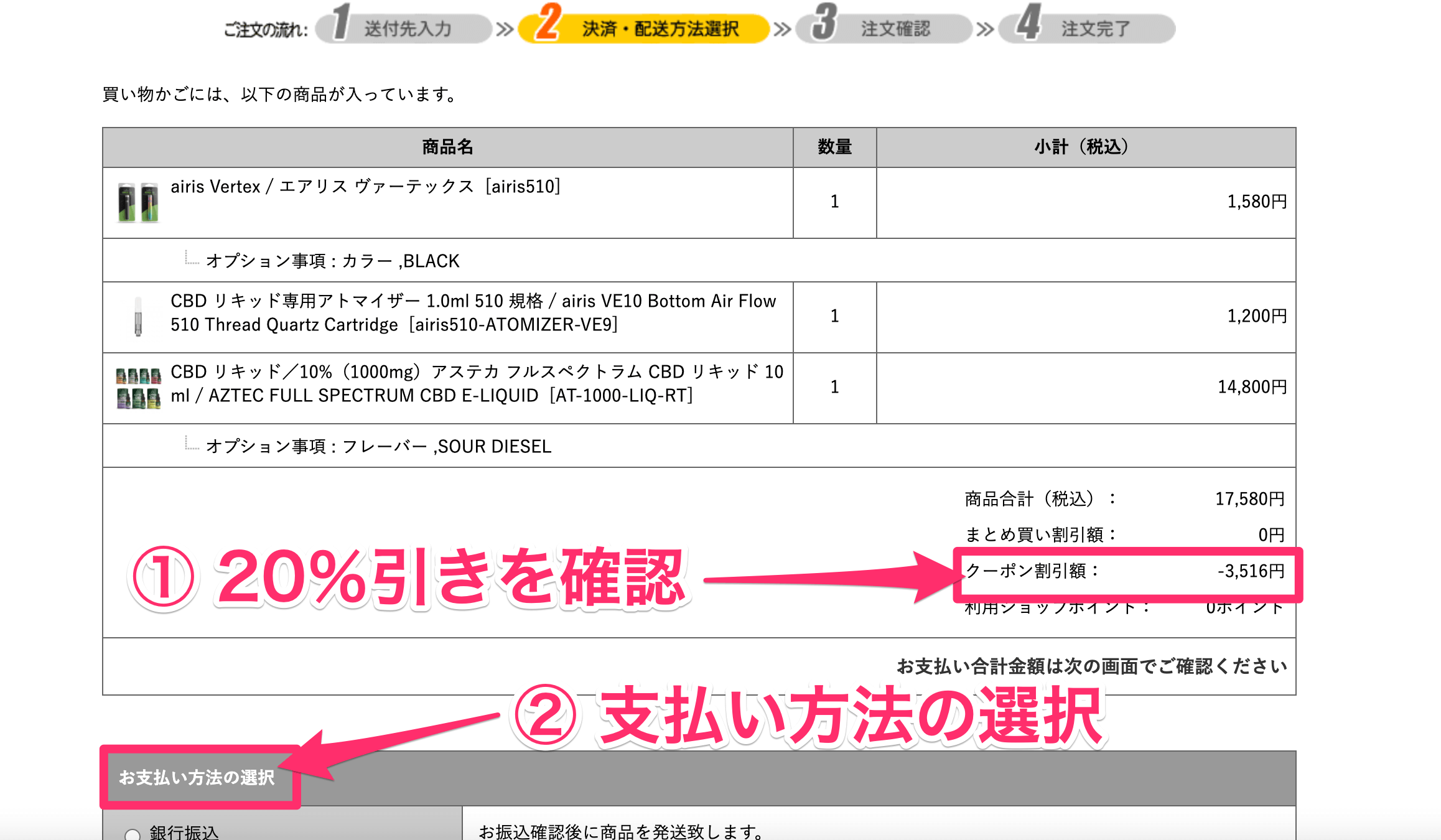
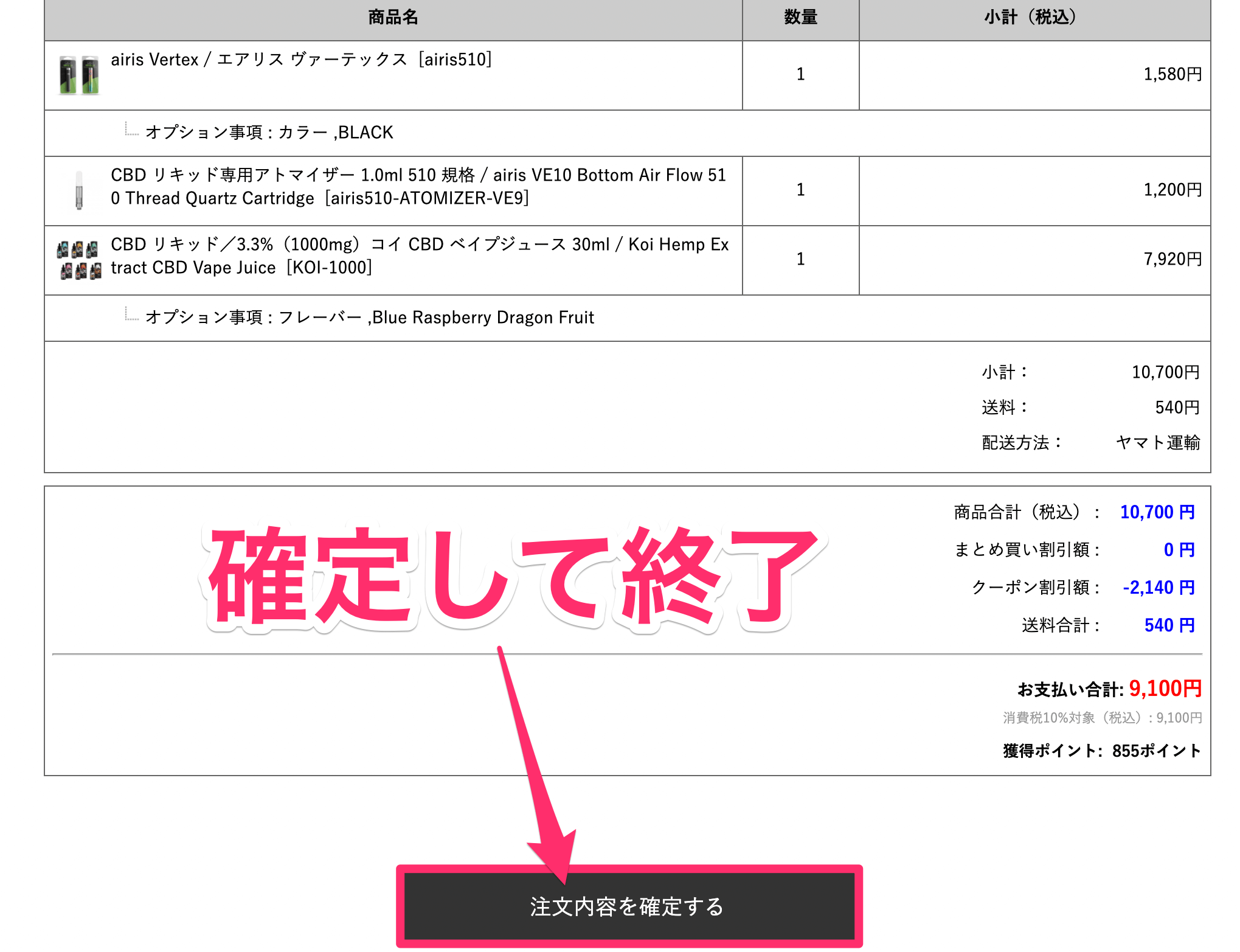
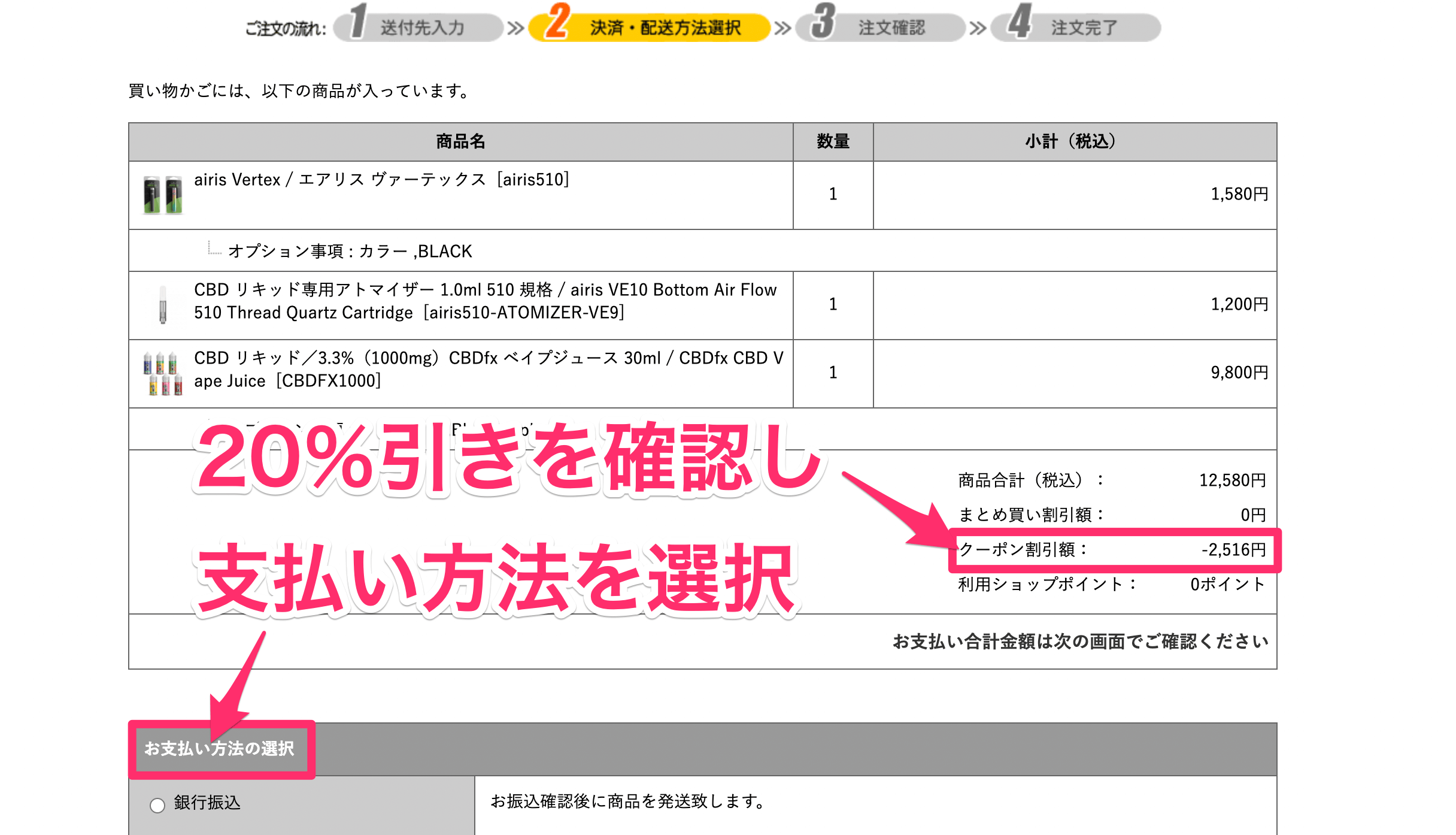
まず20%引きを確認しよう。そして、支払い方法の選択へと進んでいく。
なお、支払いには下記4種類が使用可能だ。
・銀行振り込み
・クレジットカード
・楽天Pay
・PayPay
 ファーマヘンプのリキッドを徹底レビュー!吸い心地が最高の良品【20%引きあり】
ファーマヘンプのリキッドを徹底レビュー!吸い心地が最高の良品【20%引きあり】
レビュー:PharmaHemp(ファーマヘンプ)のリキッドが初心者におすすめな理由
おすすめ2位 AZTEC(アステカ)
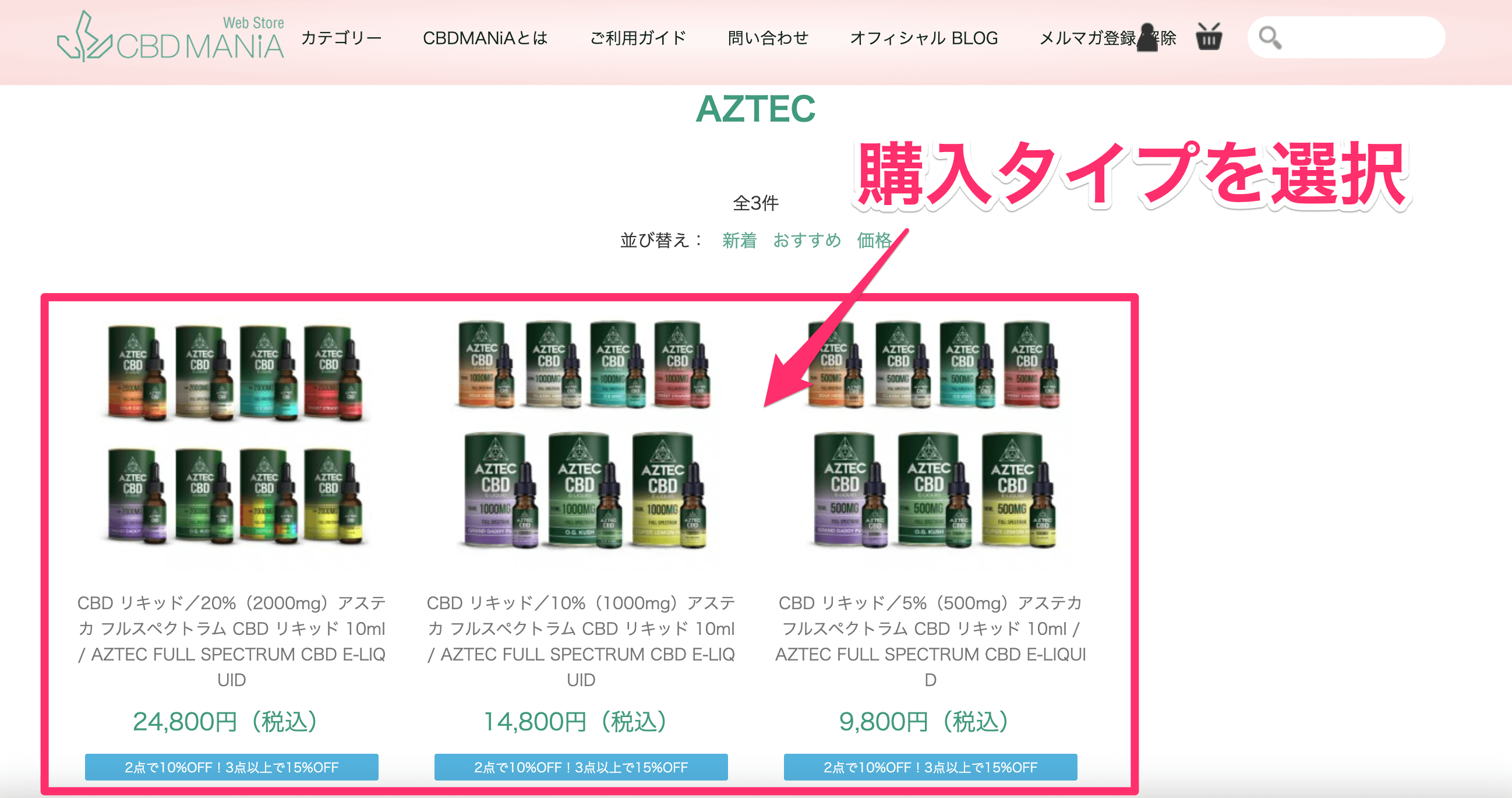
| 濃度 | 容量 | 種類 | 価格 |
| 5% | 10ml | フルスペ | 9,800円 |
| 10% | 10ml | フルスペ | 14,800円 |
| 20% | 10ml | フルスペ | 24,800円 |
おすすめ2位はアステカだ。
こちらもヨーロッパ・イギリス発のメーカーであり、言わずと知れたCBDの老舗である。
なお濃度は3パターン用意されているが、10%が断トツでおすすめだ。というのも5%ならファーマヘンプでよくて、20%は手を出しにくい価格であると思うからだ。
そしてアステカもフルスペクトラム製品のため、CBD感はいかつい程に強い。私も初めて10%のアステカを使用したときは、思わずむせてしまったほどだ。下記のリキッドの色合いを見てほしい。

このチリソースのように赤いリキッドの吸いごたえは格別だ。5%では物足りないかな・・と思う方には、ぜひ試してほしい一品である。
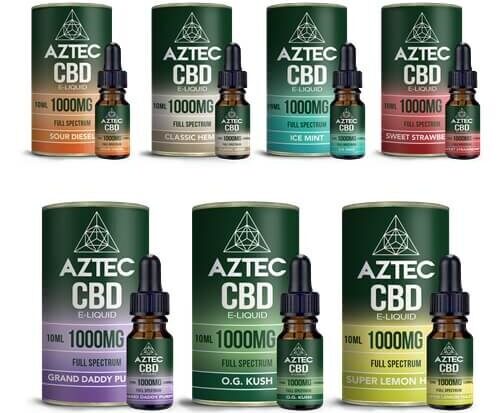
なおフレーバーは、下記の8種だ。
・アイスミント
・オージークッシュ
・サワーディーゼル
・クラシックヘンプ
・スイートストロベリー
・スーパーレモンヘイズ
・グランドダディーパープル
・スキットルズ(* 20%のみ)
「オージークッシュ」「サワーディーゼル」が個人的には美味しいと感じた。
とはいえ口コミからしてハズレの味はなかったため、気になる味を試してほしい。
ちなみに先ほど話した、20%引きクーポン(CBDMANiA20)も使える。なので仮に10%アステカを購入する場合だと、2,960円安くなる計算だ。こちらもぜひ、有効活用してほしい。


上記の、バッテリーとアトマイザーも一緒にカートに入れておこう。
20%引きは初回限定のため、まとめ買いがお得だろう。
アステカ_フルスペクトラム_CBD_リキッド_10ml___AZTEC_FULL_SPECTRUM_CBD_E-LIQUID___吸うCBD_CBDリキッド_AZTEC___CBD_専門店_CBDMANiA_オンラインショップ-3.png)
フレーバーを選択したら、「カートに入れる」をクリックする。
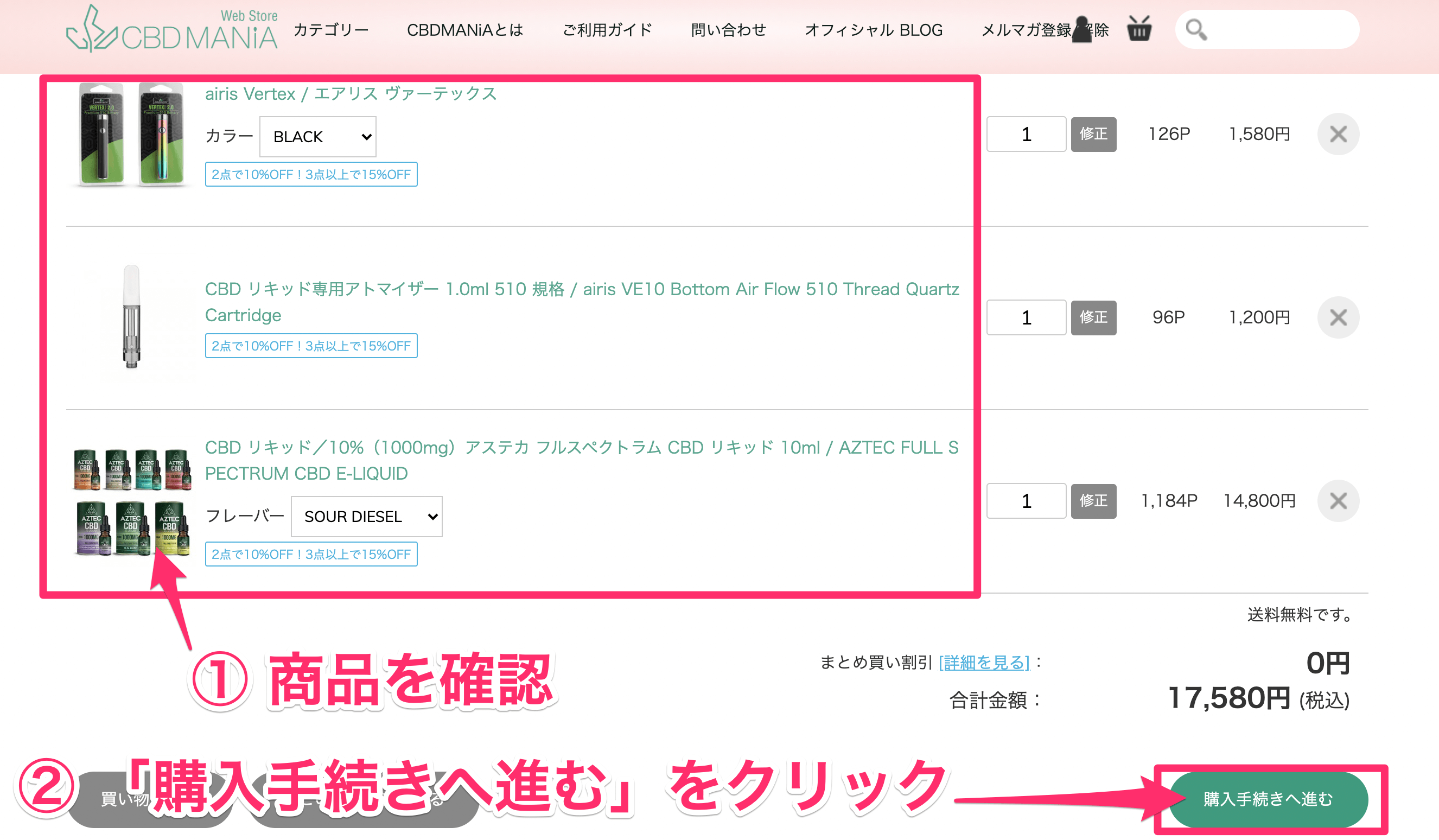
購入する商品が正しいことを確認しよう。
そして、「購入手続きへ進む」をクリックする。
ここで、「CBDMANiA20」を入力する。
入力すれば、20%引きが適用される仕組みだ。
20%引きされているかを確認しよう。そして、支払い方法の選択へと進んでいく。
なお、支払いには下記4種類が使用可能だ。
・銀行振り込み
・クレジットカード
・楽天Pay
・PayPay

 【失敗談あり】AZTEC(アステカ)のリキッドに中毒性がある訳【ハマる】
【失敗談あり】AZTEC(アステカ)のリキッドに中毒性がある訳【ハマる】
レビュー:【失敗談あり】AZTEC(アステカ)のリキッドに中毒性がある訳
おすすめ3位 +WEED(プラスウィード)
| 濃度 | 容量 | 種類 | 価格 |
| 3%~10% | 10ml | 単一 | 5,390円~16,390円 |
| 10%~60% | 10ml | フルスペ | 18,590円~73,590円 |
おすすめ3位はプラスウィードだ。
こちらはCBDでは珍しい日本のブランドであり、「安心感」が最大のポイントになる。というのも公式サイトには電話とメールでのお問い合わせがあり、ちょっとした不安ごとがあっても、すぐにオペレーターが対応してくれるからだ。
価格は1位、2位に比べて少し高めだが、「安心感」を買うと思えば安いのではないだろうか。なお現在だと、下記のキャンペーンも行われている。
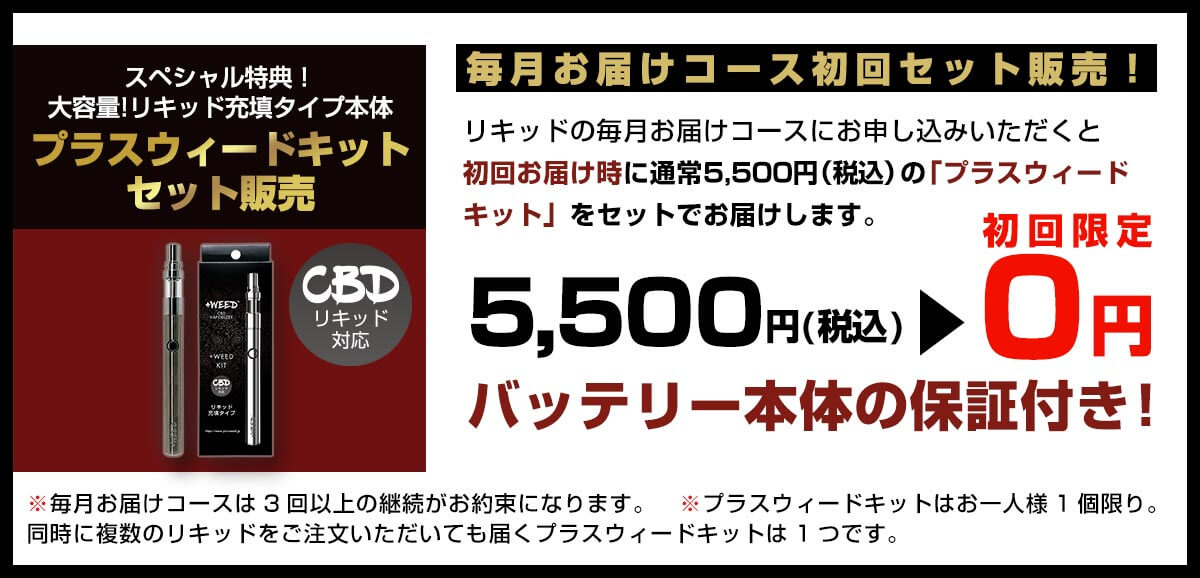
3ヶ月の継続購入が条件となるのだが、リキッドに必要な道具が無料で送られてくる。また本体保証も付いており、ここに日本会社の強みであるサポート感がにじみ出ている。
詳しくは毎月お届けコースとはに書いてあるため、参考にしてほしい。
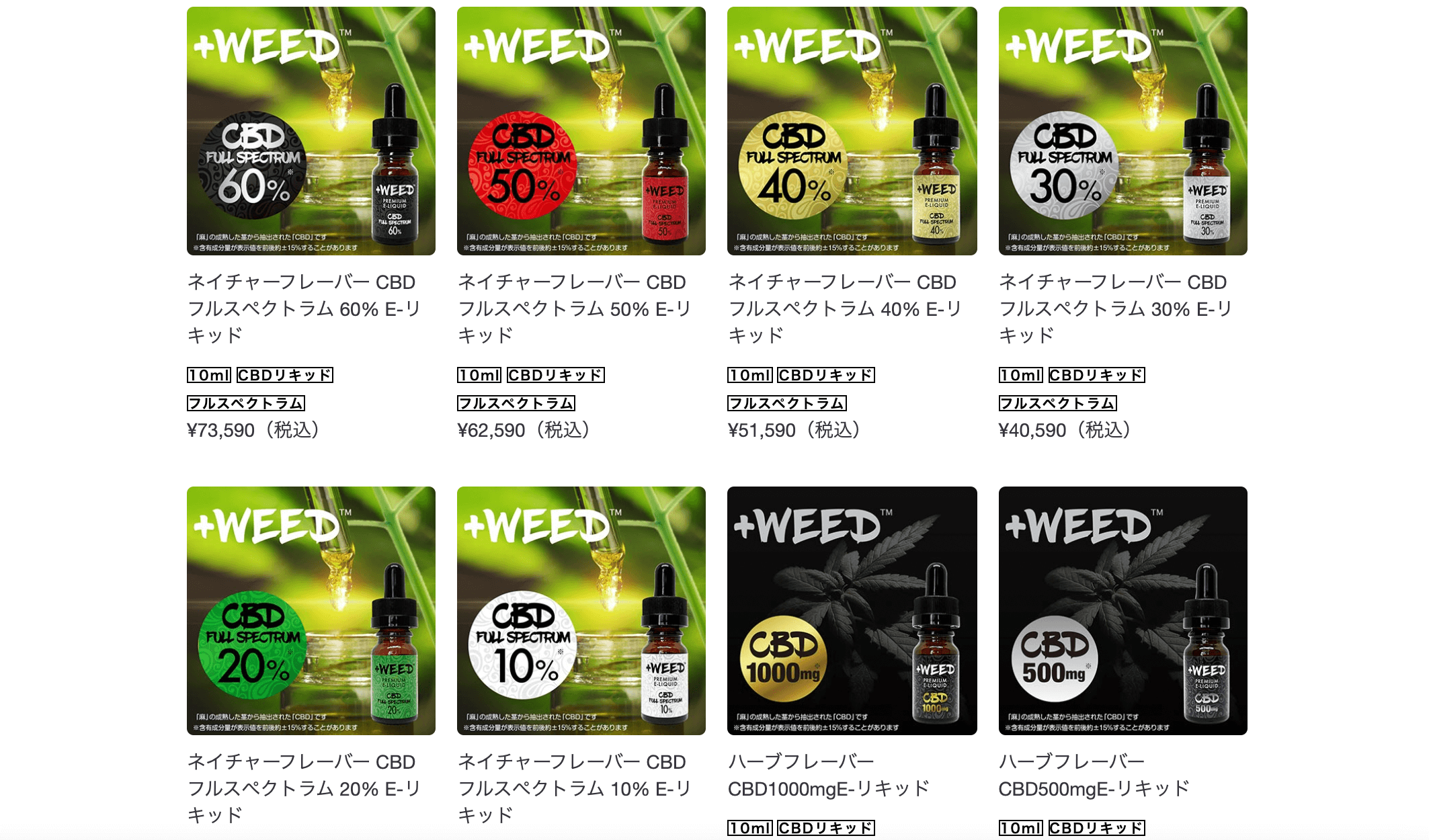
なおフレーバーは、下記の3種だ。
・ピーチシャンパン
・ハーバーフレーバー
・ネイチャーフレーバー
上記2つは単一CBD版のみ、ネイチャーフレーバーはフルスペCBDのみの提供となる。初心者の方なら単一CBD版で良いと思う。価格も手頃であり、使いやすいはずだ。
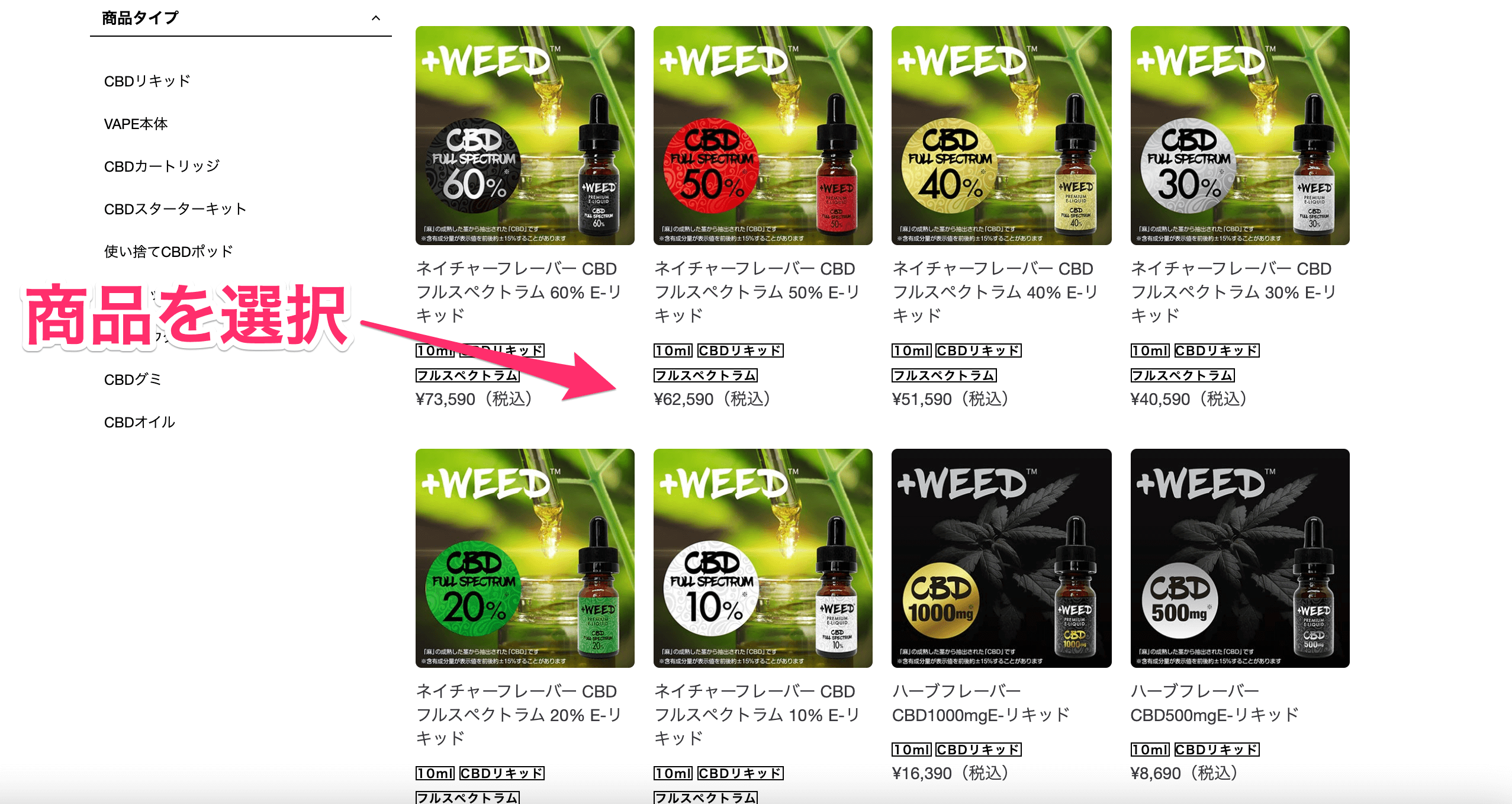

「1回購入」「毎月お届けコース」のどちらかを選択して、「カートに入れる」をクリックしよう。
なお「毎月お届けコースとは」に、継続購入の特典や詳細が書いているため、気になる方はこちらを参考にしてほしい。
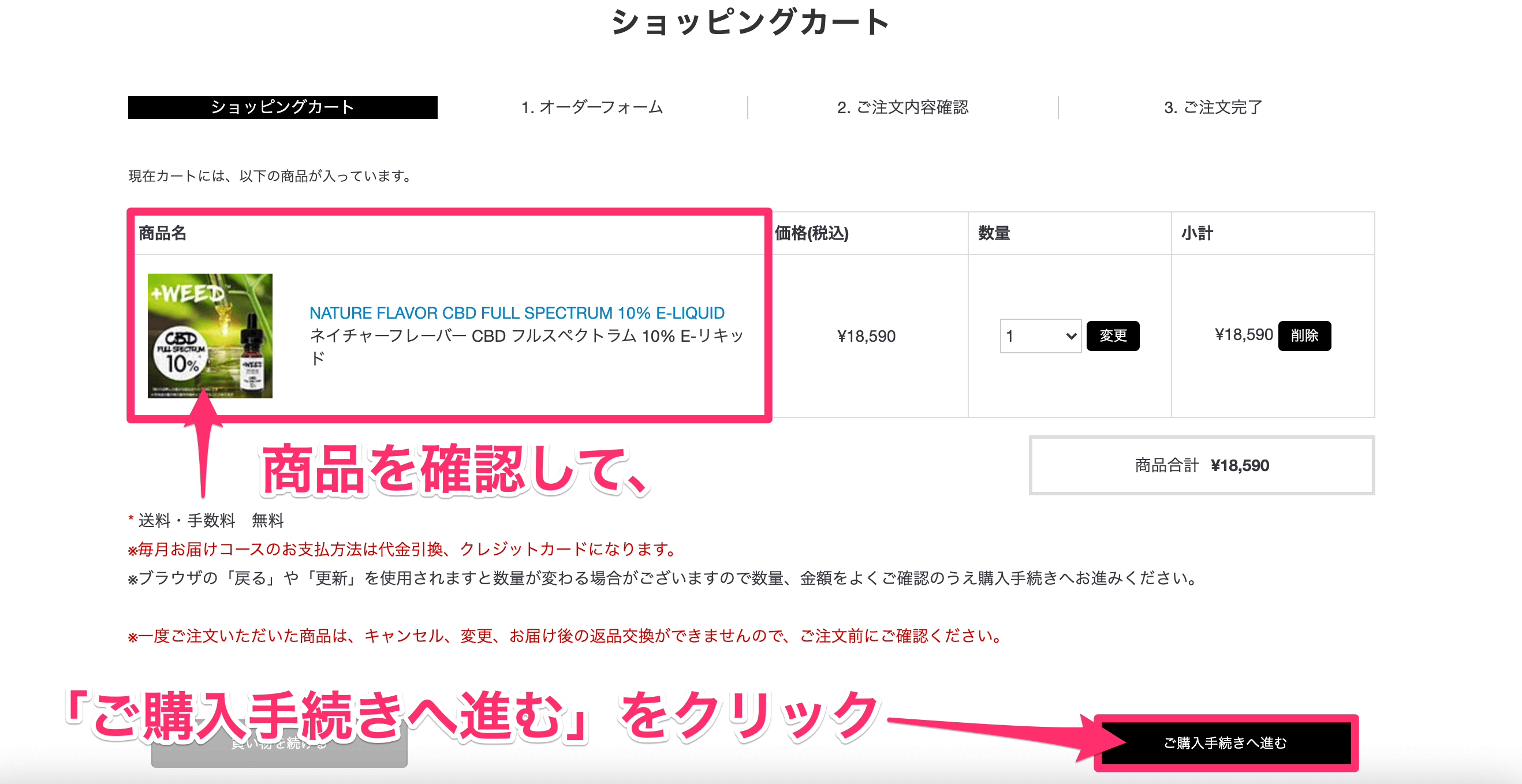
選択した商品が正しいか確認して、「ご購入手続きに進む」をクリックしよう。

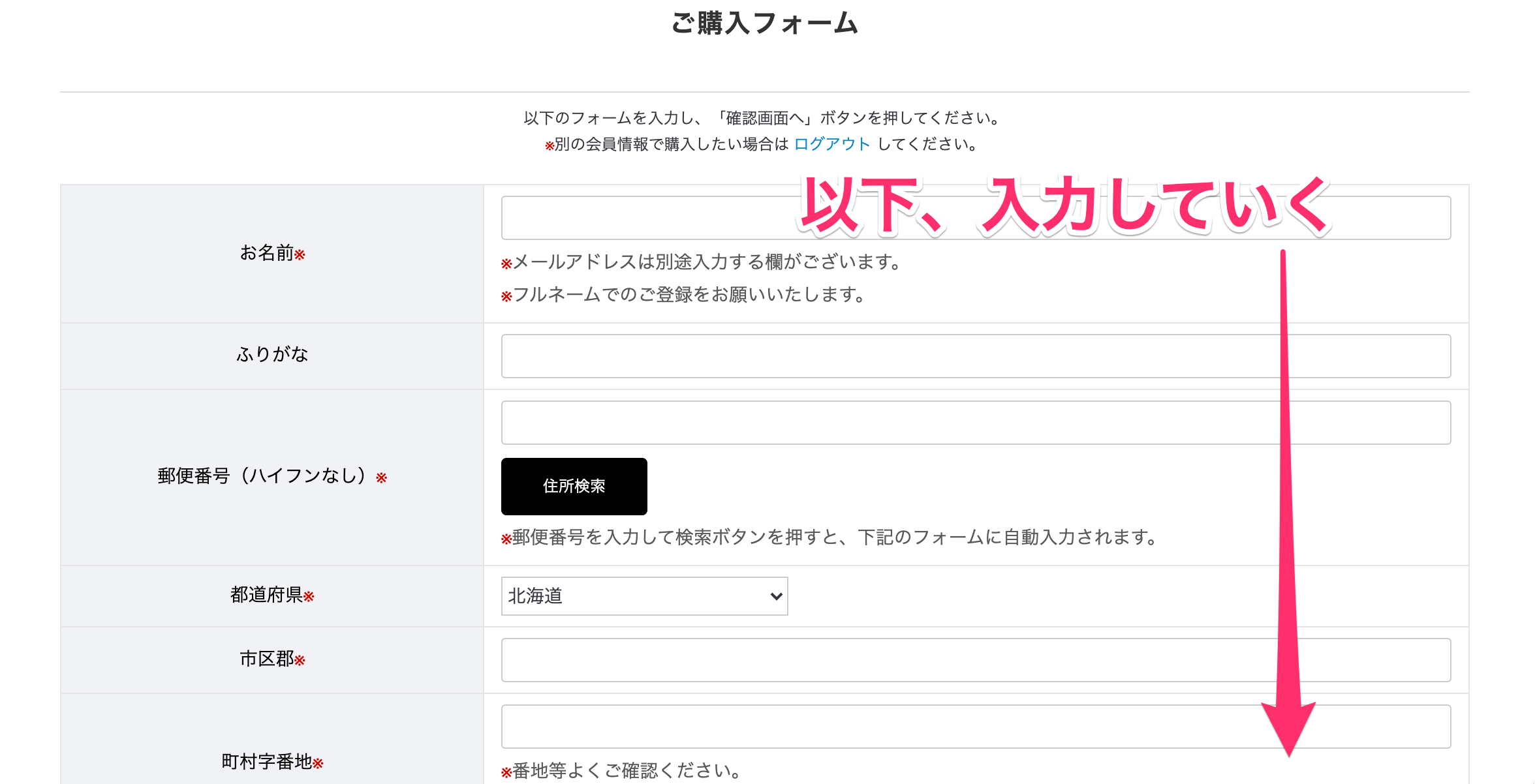
会員でない方は、ログインIDなどはムシしてOKだ。
その下の「ご購入フォーム」をネットショッピングと同じように入力していこう。
なおフォームを入力すれば、自動で会員登録をしてくれ、ポイントなどを付けてくれる便利な機能となっている。
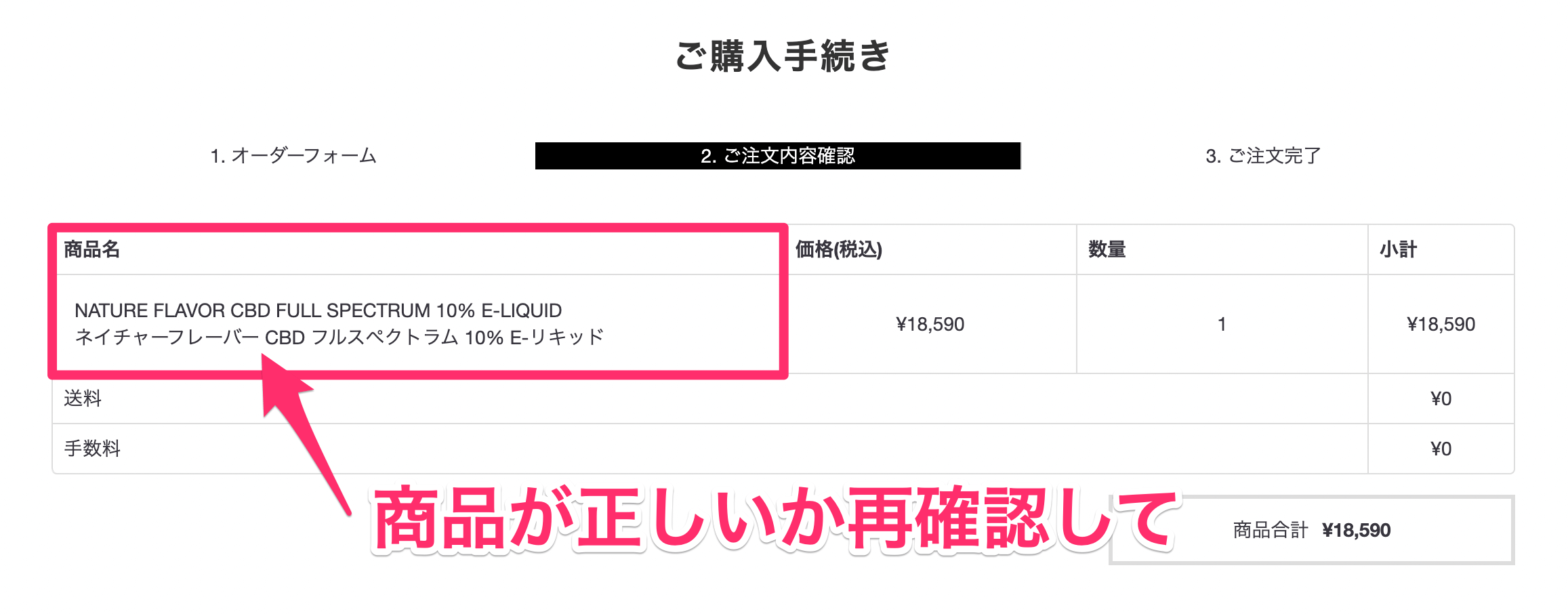
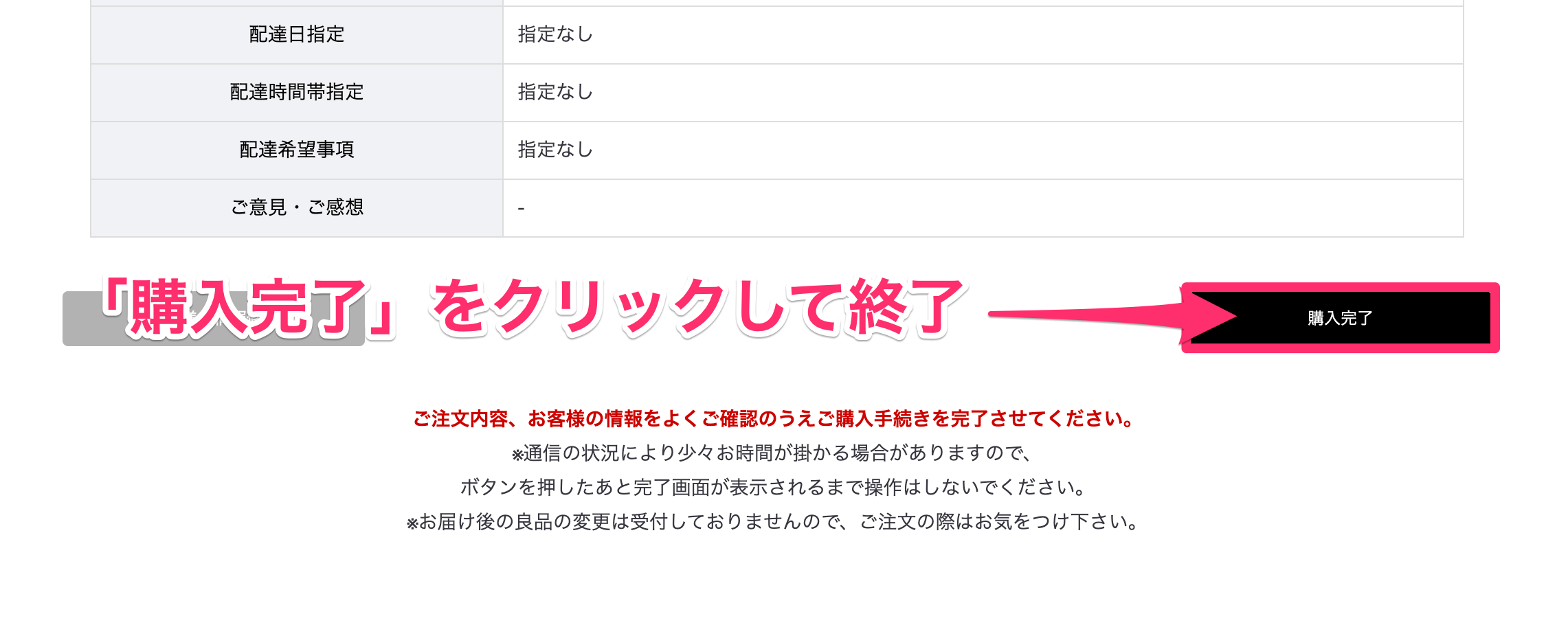
最後に、注文商品を確認し「完了」をクリックすれば終了だ
 【体験談】プラスウィードのリキッドを徹底レビュー【口コミあり】
【体験談】プラスウィードのリキッドを徹底レビュー【口コミあり】
レビュー:【体験談】プラスウィードのリキッドを徹底レビュー【口コミあり】
おすすめ4位 HERBS(ハーブス)

| 濃度 | 容量 | 種類 | 価格 |
| 1% | 15ml | 単一 | 2,200円 |
| 3% | 15ml | 単一 | 5,060円 |
| 5% | 15ml | 単一 | 7,260円 |
| 10% | 15ml | 単一 | 13,200円 |
おすすめ4位はHERBSだ。
こちらも東京に本社を置く国内メーカーであり、1%~10%という豊富なラインナップが魅力だ。
また容量が15mlのため、コスパにも優れている。私の場合だと軽く30日は持った印象があり、人によれば60日も十分に持つだろう。なお単一CBDながら吸いごたえは強く、さらにフレーバーの再現度もかなり高かったため、「高濃度かつ大容量」を求めている方にはジャストミートな製品だと感じる。
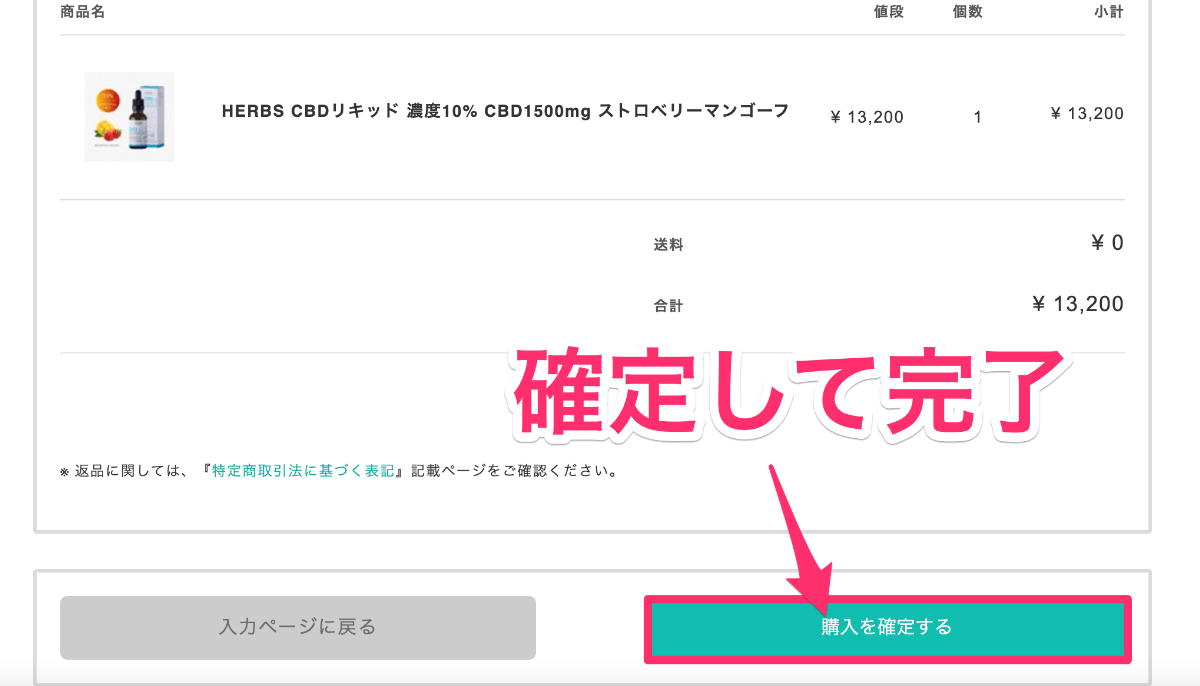
私は下記の10%(ストロベリーマンゴー)を使用したが、かなり満足できた製品だった。

なおフレーバーは、下記の5種類だ。
・ナチュラル
・メンソール
・カンナビス
・レモンティー
・ストロベリーマンゴー
ストロベリーマンゴーが甘い味わいで美味しかった。甘さを求める人にもおすすめできるリキッドだ。

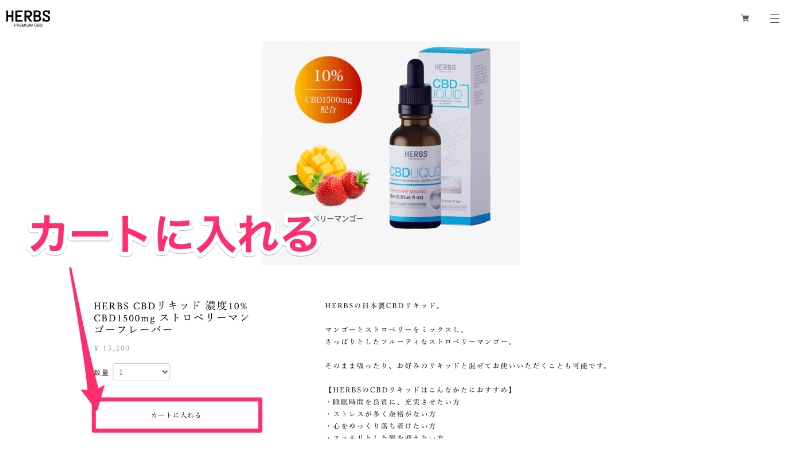
商品の詳細ページへ訪れたら、「カートに入れる」を選択しよう。
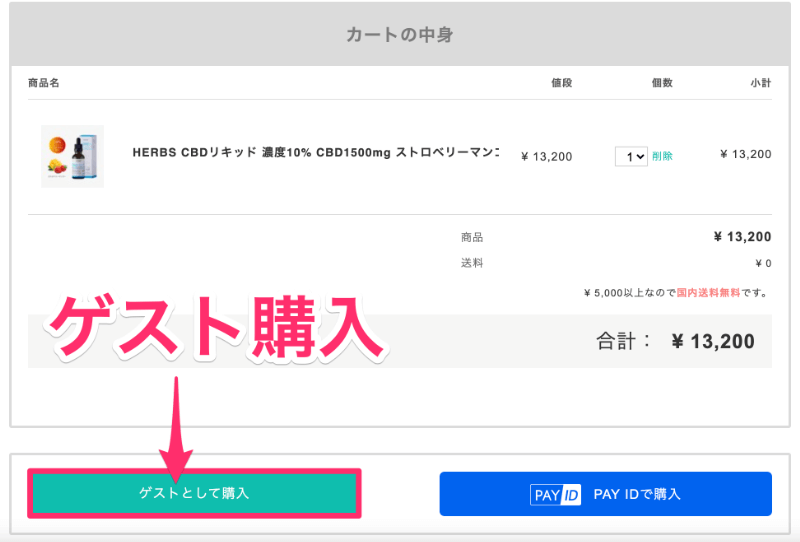
次に、購入方法を選択する。
PAY IDに登録しているなら「PAY IDで購入」を選択しよう。
とはいえ、私含めて登録してない方が多いと思うため、基本は「ゲスト購入」を選択すれば良い。

まずは、配達住所などの入力を行おう。
そして、下記のとおり決済方法も選択する。
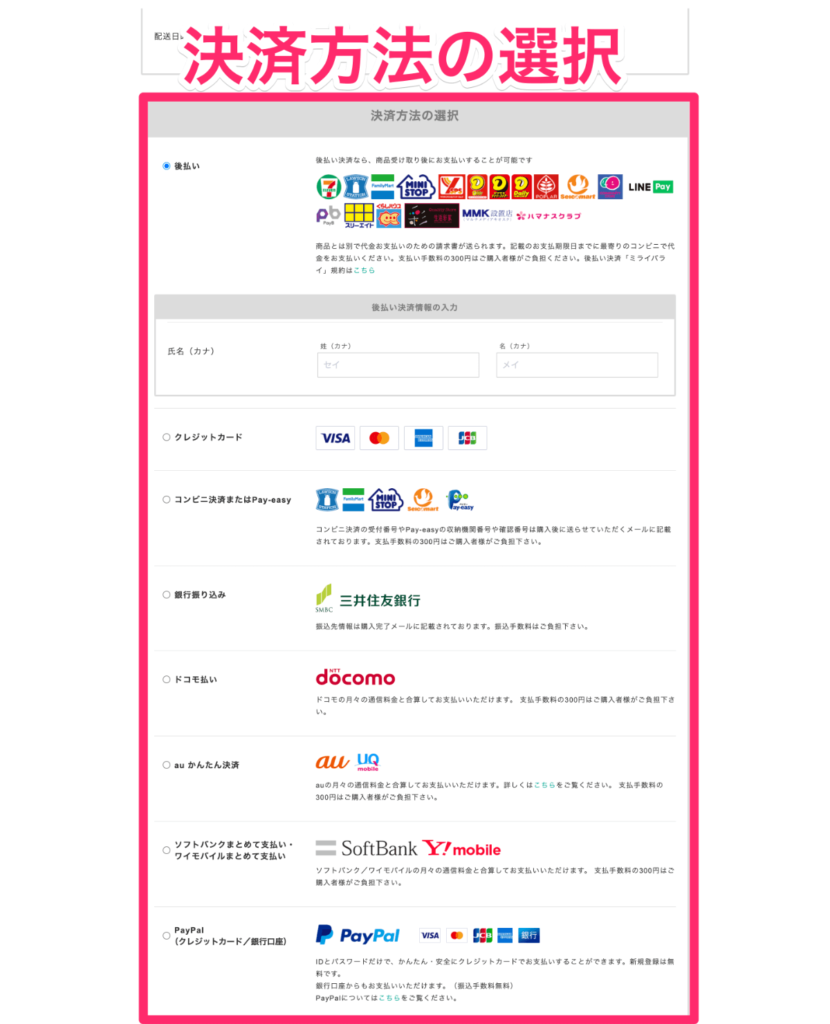
なお使用できる決済方法は次のとおり。
・後払い
・クレジットカード
・コンビニ決済またはPay-easy
・銀行振り込み
・キャリア(携帯)決済
・PayPal
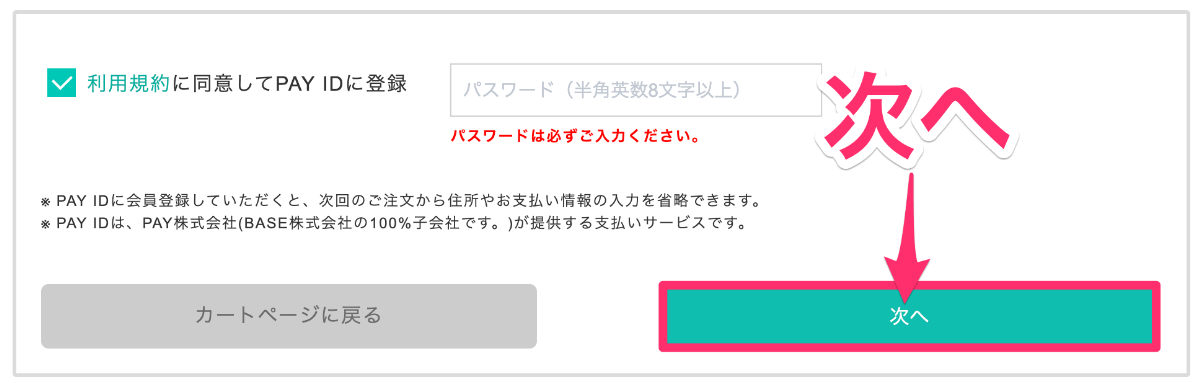
決済方法を選択すると、PAY IDの登録ができる。
とはいえここは、登録したい方だけでOKだ。
※登録すれば、次回からの購入で、住所や支払い情報などの情報を省略できるようになる。
 HERBS(ハーブス)のCBDリキッドをレビュー【結論:コスパが良すぎた】
HERBS(ハーブス)のCBDリキッドをレビュー【結論:コスパが良すぎた】
レビュー:HERBS(ハーブス)のCBDリキッドをレビュー【結論:コスパが良すぎた】
おすすめ5位 Koi(コイ)

| 濃度 | 容量 | 種類 | 価格 |
| 1.6% | 30ml | 単一 | 4,950円 |
| 3.3% | 30ml | 単一 | 7,920円 |
おすすめ5位はKoiだ。
こちらは鯉(こい)をモチーフとしたアメリカの製品であり、CBDの祭典「CBDエキスポ」では最優秀賞も受賞した人気のメーカーだ。
そしてハーブスの15mlも上回る「30ml型」の大容量のため、「とにかくたくさん吸いたい!」と思う方にはピッタリだろう。なお濃度自体は低めだが、30mlもあるため、モクモクと吸っても余裕で1ヶ月は持つ感覚だ。そこまでのスモーカーではない友人はこれ一本で3ヶ月も持ったとも言っていた。
またフレーバーの再現度も高く、味わいに凝りたい方にはぜひおすすめしたいリキッドである。

そしてそんなフレーバーは、下記の6種が用意されている
・ピンクレモネード
・グリーンアップルサワー
・バニラキャラメルカスタード
・ストロベリーミルクシェイク
・フレーバーレスコイホワイト
・ブルーラズベリードラゴンフルーツ
「フレーバーレスホワイト」以外は甘い味わいのため、こちらも好きな果物の種類があるなら、そこから選ぶのが良いだろう。
ちなみに、先ほど話した20%引きクーポン(CBDMANiA20)も使える。

上記の、バッテリーとアトマイザーもカートに入れておこう。
それぞれ、販売ページのリンクも用意しておく。
コイ_CBD_ベイプジュース_30ml___Koi_Hemp_Extract_CBD_Vape_Juice___吸うCBD_CBDリキッド_Koi_CBD___CBD_専門店_CBDMANiA_オンラインショップ-e1621404332761.png)
フレーバーを選択したら、「カートに入れる」をクリックする。
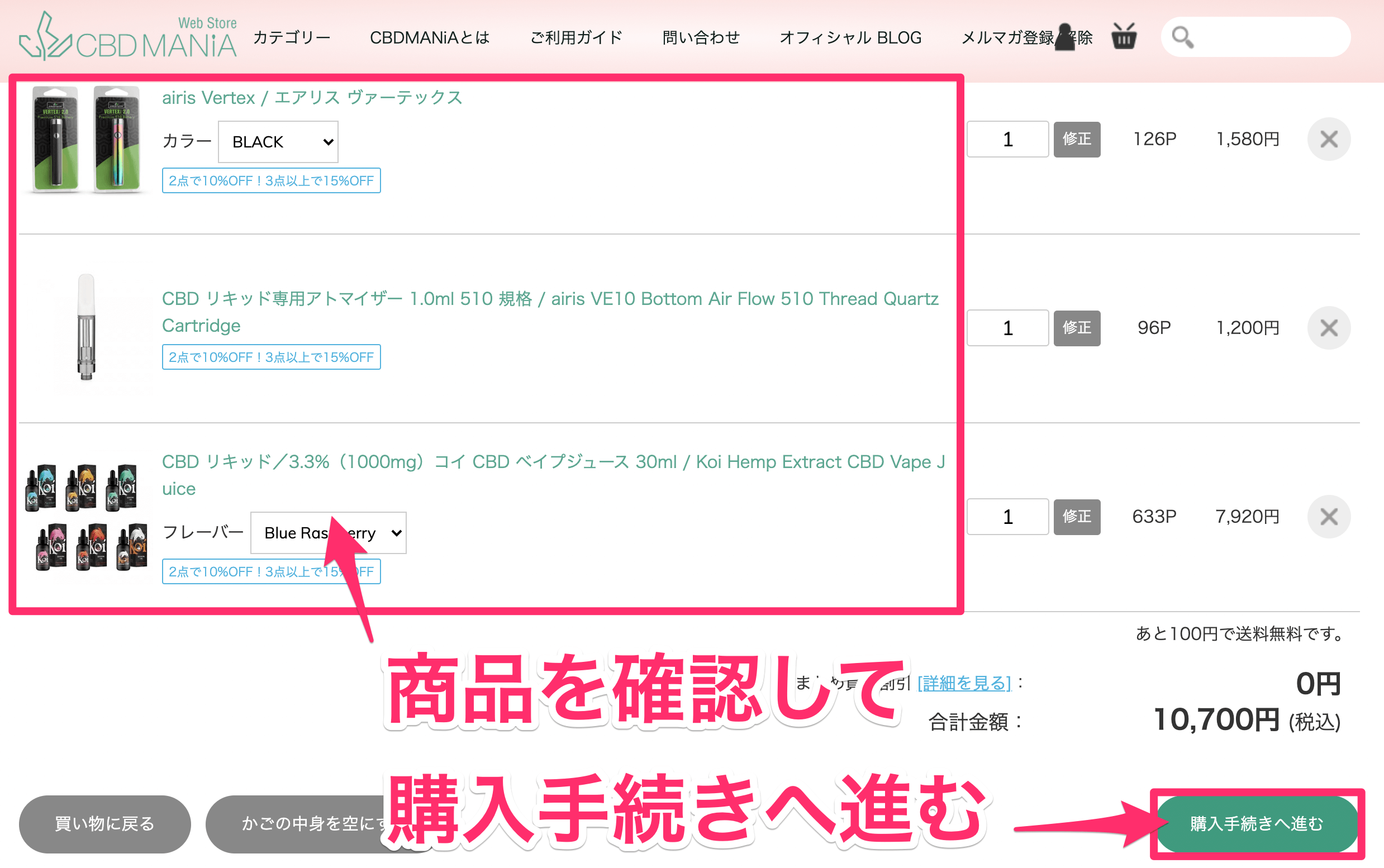
購入する商品が正しいことを確認しよう。
そして、「購入手続きへ進む」をクリックする。
ここで、「CBDMANiA20」を入力する。
入力すれば、20%引きが適用される仕組みだ。

20%引きされているかを確認しよう。そして、支払い方法の選択へと進んでいく。
なお、支払いには下記4種類が使用可能だ。
・銀行振り込み
・クレジットカード
・楽天Pay
・PayPay
 【体験談】KoiのCBDリキッドは「チル向け」の傑作だった話【レビュー】
【体験談】KoiのCBDリキッドは「チル向け」の傑作だった話【レビュー】
レビュー:【体験談】KoiのCBDリキッドは「チル向け」の傑作だった話
おすすめ6位 CBDfx

| 濃度 | 容量 | 種類 | 価格 |
| 1.6% | 30ml | 単一 | 7,480円 |
| 3.3% | 30ml | 単一 | 11,680円 |
おすすめ6位はCBDfxだ。
こちらもKoi同様アメリカ発のメーカーであり、最近少しずつ人気を集めているブランドだ。なお有名アスリートを中心に、男性女性問わず使用する方が増えてきた印象がある。
>>参考:トップアスリートがCBDを愛用する理由
ネット通販以外でも、2021年の6月には東京のOIOI(マルイ)に設けられたCBDコーナーにもfxの商品が並んでおり、知名度は徐々に高まっている。
ちなみにボトルはユニコーン型(先端がとがっている種類)のため、スポイトのリキッドに比べると、注入作業が比較的簡単だった印象がある。

なおフレーバーは、下記の6種類だ。
・ブルーラズベリー
・ストロベリーミルク
・ストロベリーキウイ
・フルーティーシリアル
・レインボーキャンディー
・ワイルドウォーターメロン
なおCBD濃度が低い分、フレーバーにかなり力を入れている印象があった。正直、フレーバーの味だけならCBDfxが1番だと思えるくらいだ。
どれも非常に甘い味わいのため、ここは好みの果物から選ぶのが良いと思う。甘めな香りが好きな方は、ぜひ試してほしい。
CBDfx_ベイプジュース_30ml___CBDfx_CBD_Vape_Juice___吸うCBD_CBDリキッド_CBDfx___CBD_専門店_CBDMANiA_オンラインショップ-1.png)
上記の、バッテリーとアトマイザーもここでカートに入れておこう。
それぞれ、販売ページのリンクも用意しておく。
購入する商品が正しいことを確認しよう。
そして、「購入手続きへ進む」をクリックする。
ここで、「CBDMANiA20」を入力する。
入力すれば、20%引きが適用される仕組みだ。
20%引きされているかを確認しよう。そして、支払い方法の選択へと進んでいく。
なお、支払いには下記4種類が使用可能だ。
・銀行振り込み
・クレジットカード
・楽天Pay
・PayPay
 【比較あり】CBDfxのリキッドにハマる訳【結論:甘みが最高クラス】
【比較あり】CBDfxのリキッドにハマる訳【結論:甘みが最高クラス】
レビュー:【比較あり】CBDfxのリキッドにハマる訳【結論:甘みが最高クラス】
おすすめ7位 りきっどや

| 濃度 | 容量 | 種類 | 価格 |
| 3.3% | 30ml | 単一 | 3,979円 |
| 10% | 10ml | 単一 | 3,979円 |
おすすめ8位は、りきっどやだ。
こちらは電子タバコ(ベイプ)を使う人なら一度は聞いたことがあるメーカーだろう。リキッドを扱う国内の老舗のメーカーであり、フレーバーがとにかく美味しいことで有名なのだ。
なお販売タイプはどちらもCBD含有量が1000mgであり、容量が違う。そのため濃いCBDを吸いたい方は10mlを、モクモクと吸いまくりたい方は30mlといった形で、好みのタイプを選ぶことができる。
そしてりきっどやもユニコーン型のボトルであり、注入が簡単だ。電子タバコ界ではTOPクラスの人気を獲得しているだけあり、価格面や味の再現度も素晴らしいものだった。

そんな”りきっどや”が扱うフレーバーは、下記の6種だ。
・もも極
・メロン極
・みかん極
・メンソール
・青りんご極
・マスカット極
名前の「極」にふさわしい再現性にこだわったリキッドのため、フレーバー重視の方にはおすすめだ。
個人的には「メロン極」がヤバかったので、決められない方は、ぜひ試してほしい。
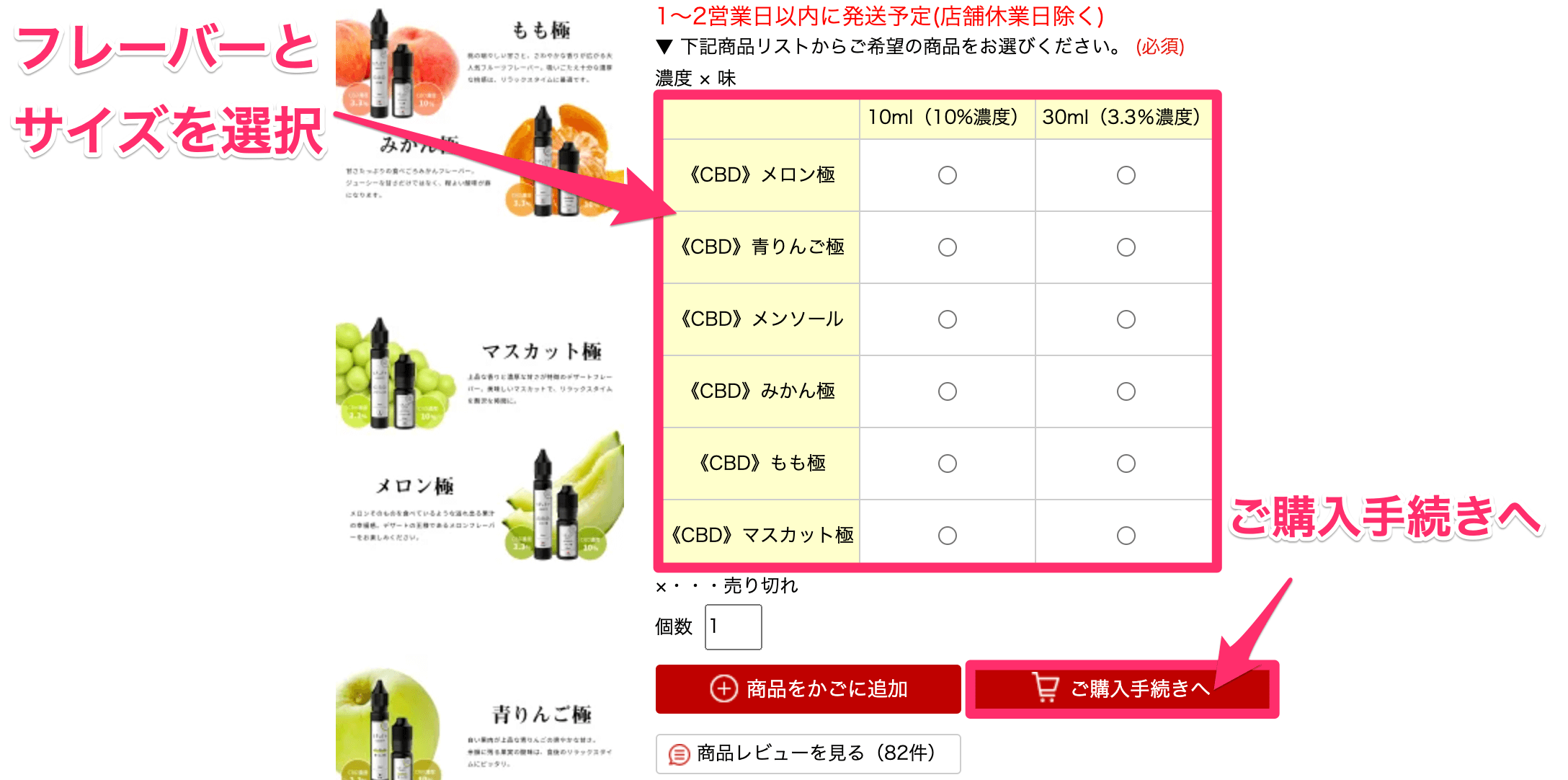
まずはフレーバーを選択し、ご購入手続きへを選択しよう。
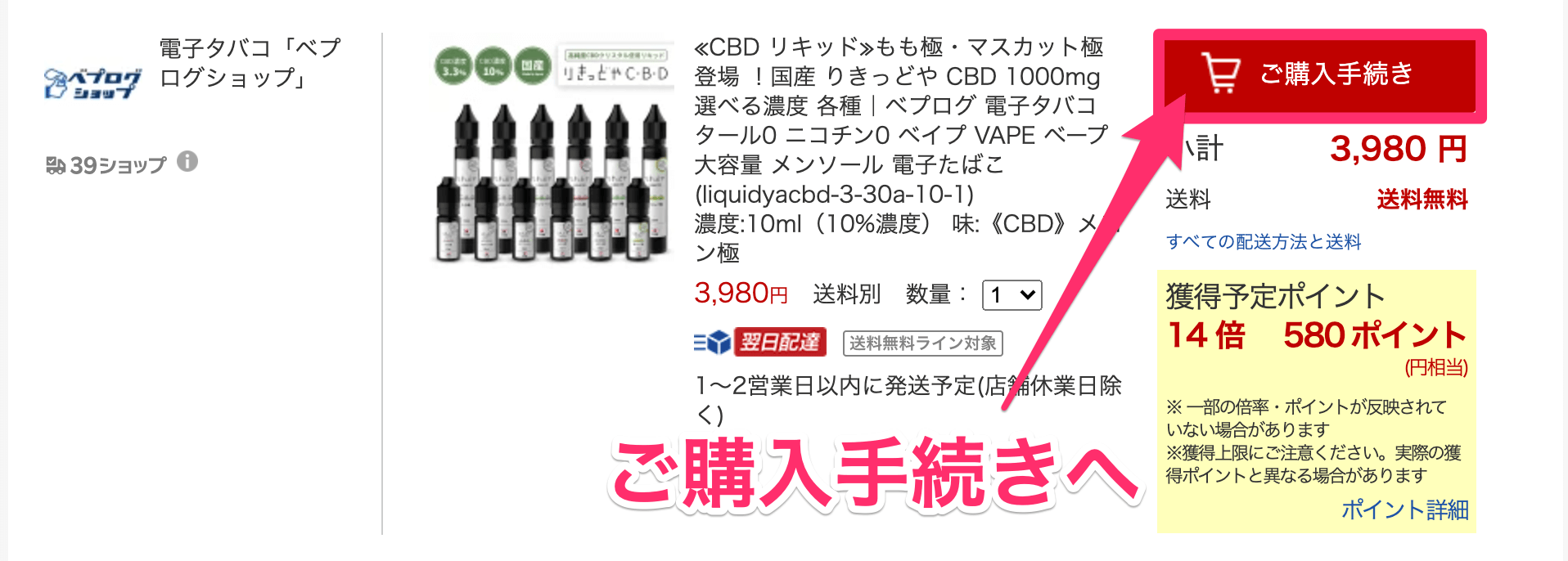
上記の画面になるため、またご購入手続きへと進もう。
そして注文を確定して終了だ。
 【レビュー】りきっどやのCBDリキッドが神作な理由【口コミあり】
【レビュー】りきっどやのCBDリキッドが神作な理由【口コミあり】
レビュー:りきっどやのCBDリキッドが神作な理由【口コミあり】
おすすめ8位 AVIDA(アヴィダ)

| 濃度 | 容量 | 種類 | 価格 |
| 3.3% | 30ml | 単一 | 7,980円 |
おすすめ8位は、AVIDAだ。
AVIDAの特徴は、独自の技術によってCBDをナノ乳化し、「生体利用率(バイオアベイラビリティ)」を最大化しているところにある。

生体利用率とは、成分をどれだけ効率よく吸収できているかを表す数字だ。つまりこの数字が高いほど、CBDをムダなく吸収できる。
またボトルはユニコーン型であり、こちらもリキッドを注ぎやすいモデルだ。

とにかく「品質」にこだわっているのがポイントであり、価格は高めだが購入して損はないだろう。
なおフレーバーは脅威の14種類であり、詳細はレビュー記事にまとめておこう。王道から珍味なフレーバーまで用意されていたため、選択肢が豊富だ。


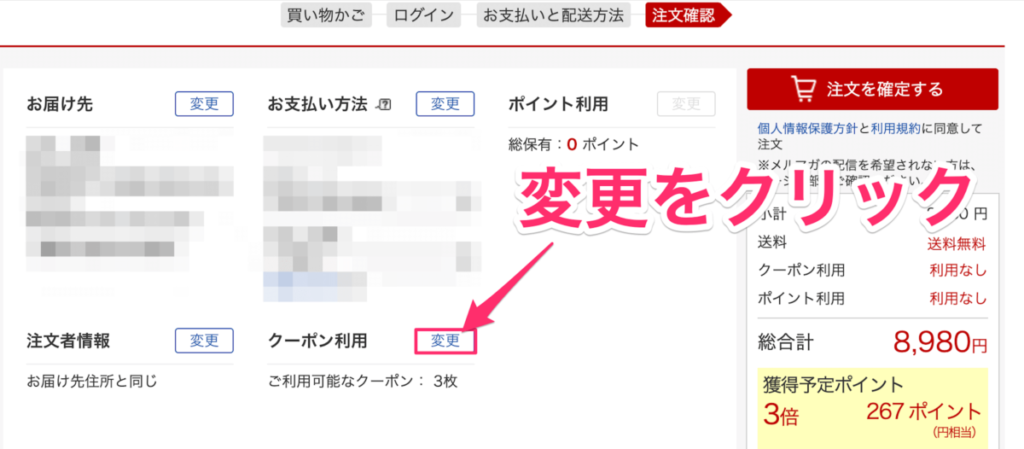
上記のクーポンを選択しよう。
-1.png)
そして、「このクーポンを使う」を選択しよう。
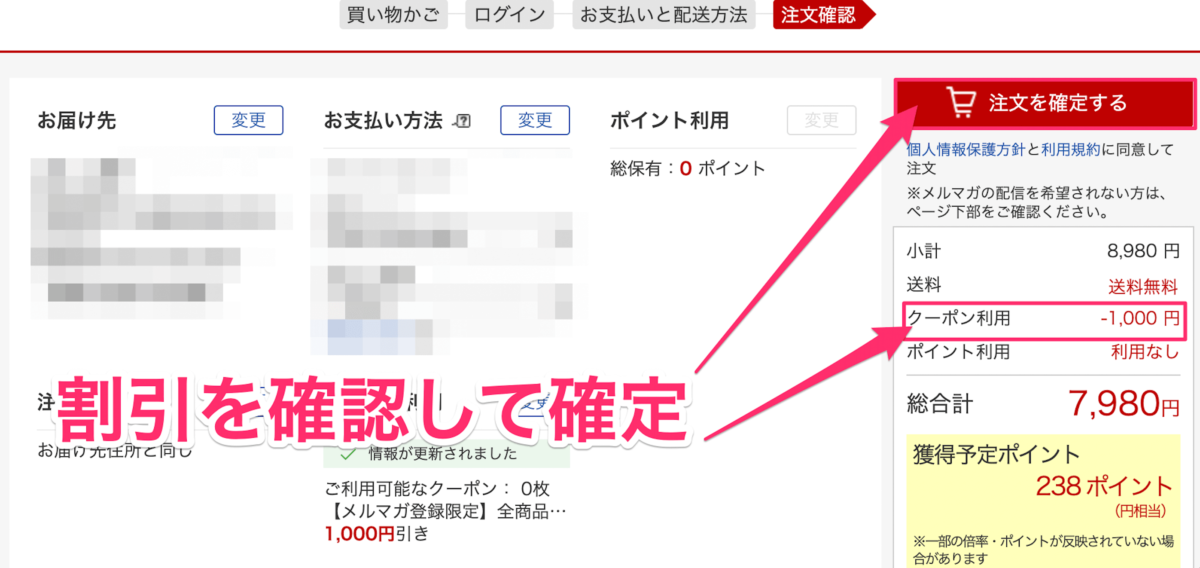
後は、いつものとおり。
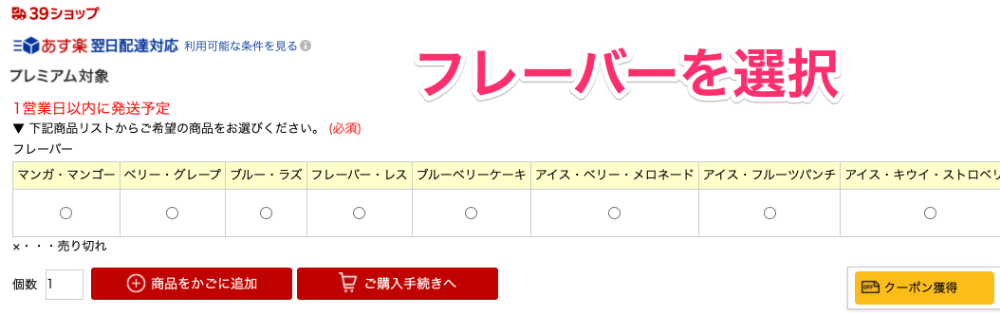
好きなフレーバーをかごに追加して、購入手続きへと進もう。
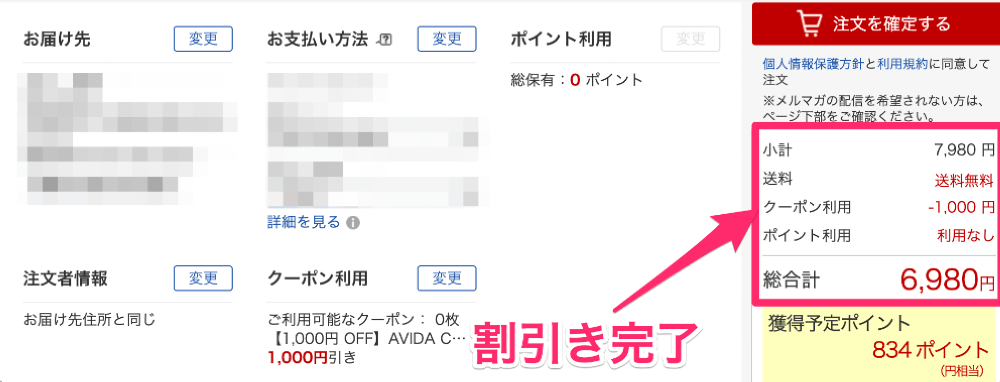
上記のとおり、1,000円引きとなっている。
正直お得すぎるので、クーポンが使える期間内に使っておくのが得策だろう。
 【レビュー】AVIDAのCBDリキッドを使ってみた結果【結論:絶妙なうまさ】
【レビュー】AVIDAのCBDリキッドを使ってみた結果【結論:絶妙なうまさ】
レビュー:AVIDAのCBDリキッドを使ってみた結果【結論:絶妙なうまさ】
おすすめ9位 キャナテック

| 濃度 | 容量 | 種類 | 価格 |
| 5% | 10ml | ブロード | 4,980円 |
| 10% | 10ml | ブロード | 8,980円 |
おすすめ9位は、キャナテックだ。
こちらも神奈川に拠点を置く国内メーカーであり、国内自社工場で徹底的な品質管理を行っている。
またキャナテックのリキッドには「テルペン」も豊富に配合されており、フレーバーの味がより一層引き立てられている。

テルペンとは、植物の精油成分である。
香水やアロマセラピーなどで使用されており、いわゆる「良い香り」を出してくれている物質だ。
なお「ブロードスペクトラム型」のCBDであり、フルスペクトラムと単一CBDとの違いは下記のとおり。
上記のとおり、フルスペクトラムほどではないが単一CBDのリキッドより吸いごたえを強く感られる。そのためキック感を求める方は、このブロード型もしくはフルスペ型にするのが最適だ。
ちなみに、フレーバーは下記の3種。
・ナチュラル
・オージークシュ
・ストロベリーコフ
私は「ナチュラル」を試したが、変なクセがあるわけではなかったため、万人におすすめできると感じた。
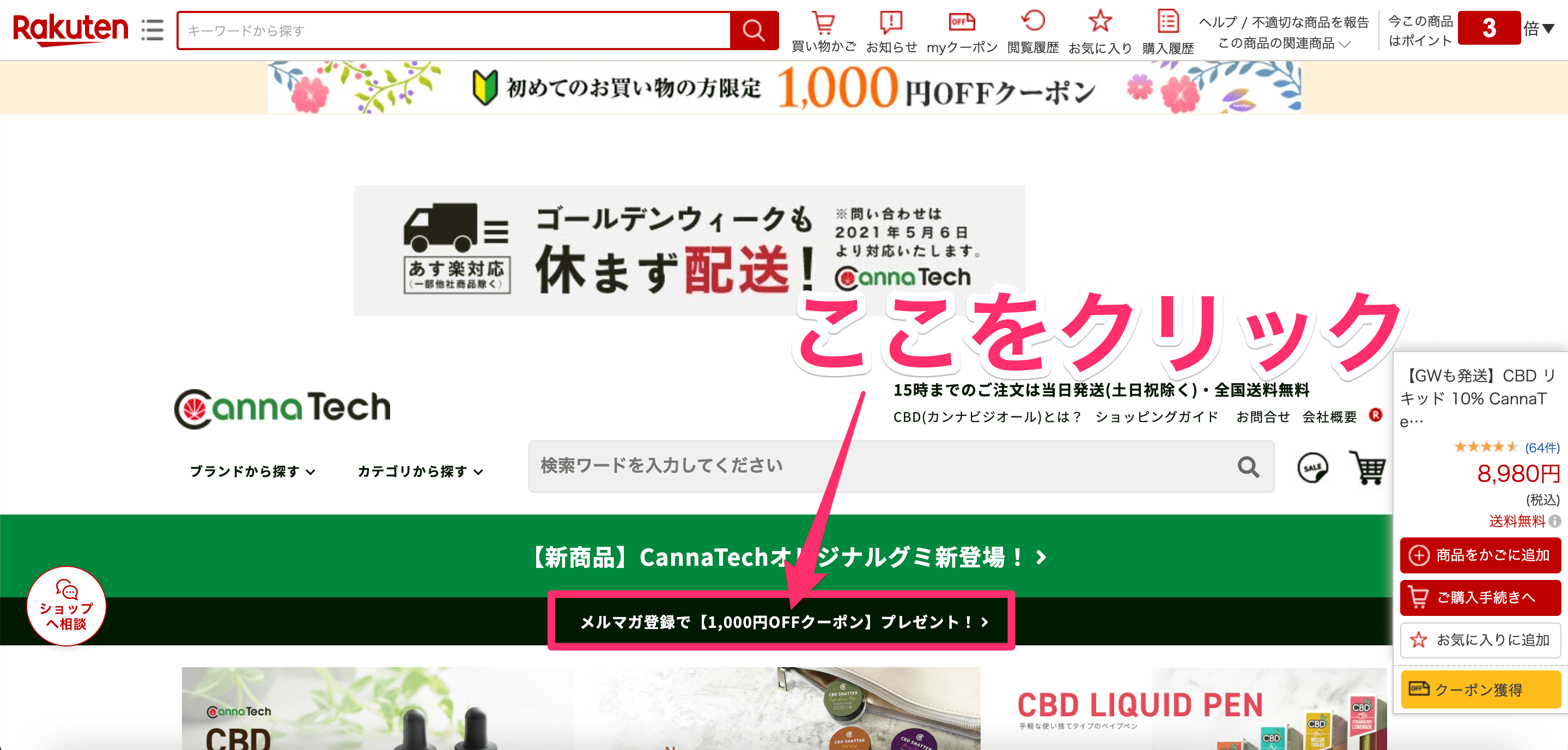

次にメールアドレスの入力だ。
そして、「登録してクーポンをGET」をクリック。
.png)
上記の画面になれば、もうクーポンは取得できている。
後は、いつものようにカートに入れる作業をしていき、購入の最終画面まで進んでいこう。
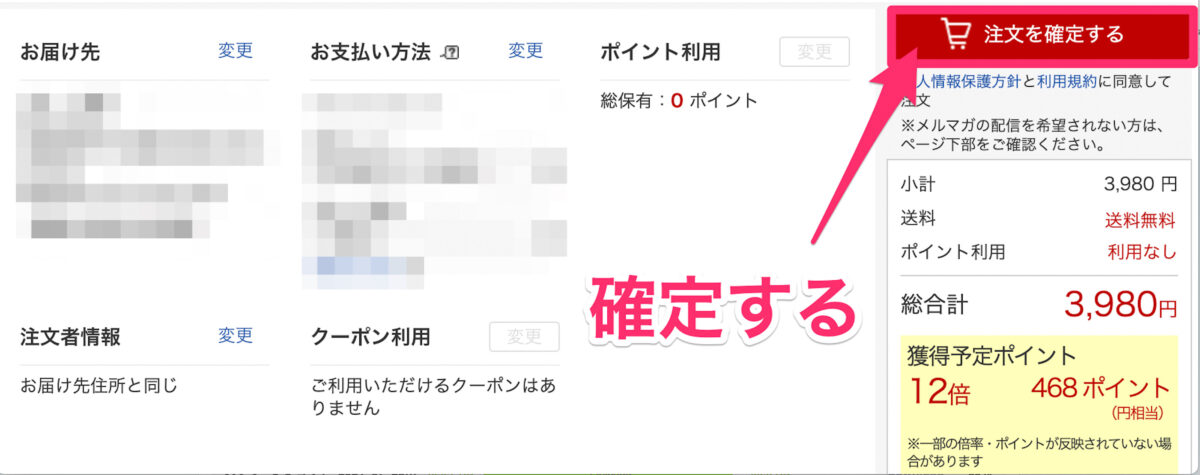
購入手続きの最終段階までいくと、上記の画面になるはずだ。
ここで、「クーポン利用」をクリックして、先ほど取得したクーポンを利用しよう。
すると、1000円引きがしっかりと行われている。
あとは到着を待つのみだ。
 CannaTech(キャナテック)のリキッドとカートリッジを使ってみた!
CannaTech(キャナテック)のリキッドとカートリッジを使ってみた!
レビュー:CannaTech(キャナテック)のリキッドとカートリッジを使ってみた!
おすすめ10位 月の葉

| 濃度 | 容量 | 種類 | 価格 |
| 1% | 10ml | 単一 | 1,480円 |
| 5% | 10ml | 単一 | 4,480円 |
| 10% | 10ml | 単一 | 7,980円 |
おすすめ10位は、月の葉だ。
こちらも国内メーカーであり、ドンキホーテなどでも販売されている。そんな月の葉の強みは、「吸いやすさ」だ。単一CBDのためCBD感はうすいが、初心者にとっては扱いやすいリキッドという印象がある。

また月の葉が用意するフレーバーは、下記の5種。
・ダブルマンゴー
・ナチュラルヘンプ
・ハードメンソール
・ジューシーピーチメンソール
・プレミアムグレープメンソール
なお私はすべて試してみた。特に「ダブルマンゴー」が美味しかったため、悩む方にはそちらをおすすめしたい。またレビュー記事では全てを試した結果も書いたため、ぜひ参考にしてほしい。
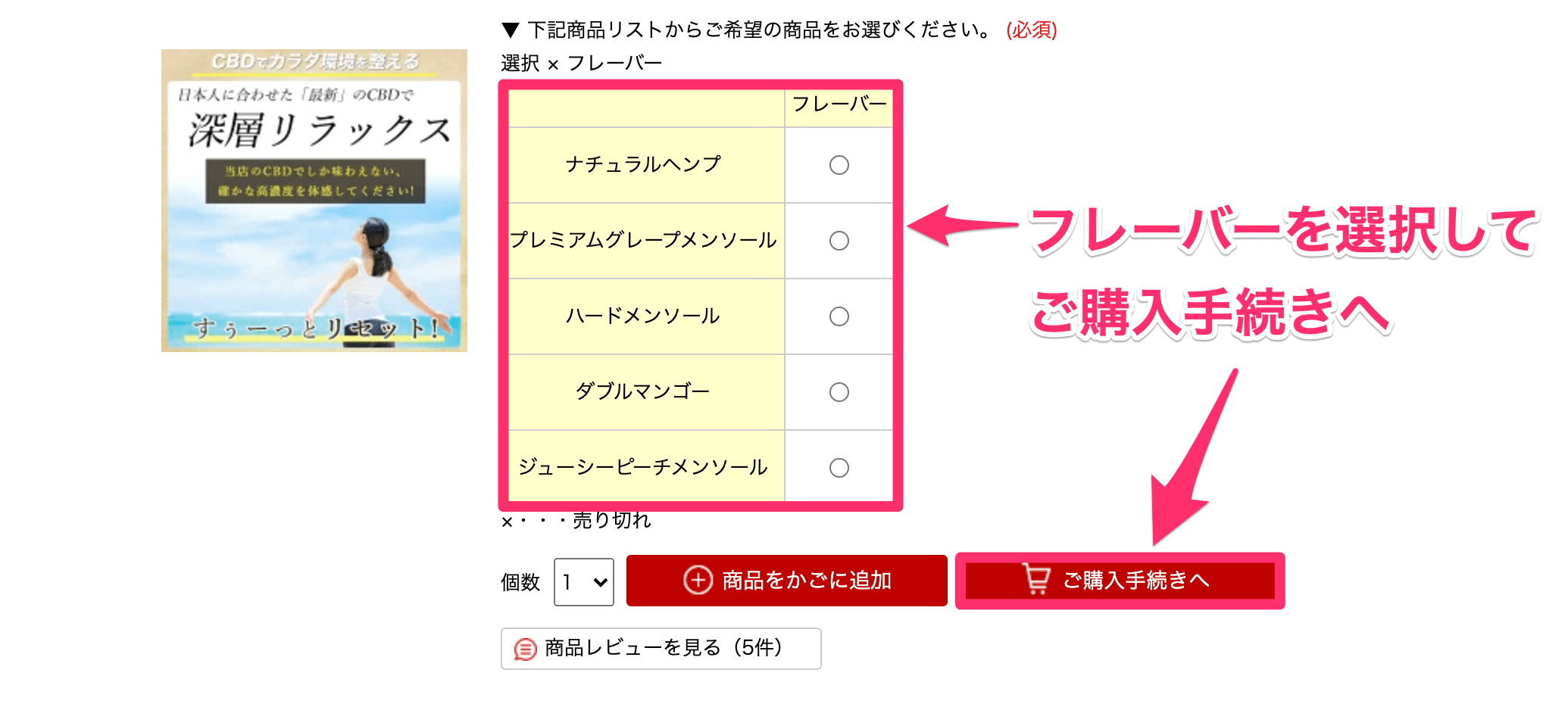
まずは、フレーバーを選択してご購入手続きを選択しよう。

上記の画面になるため、もう一度ご購入手続きを選択しよう。
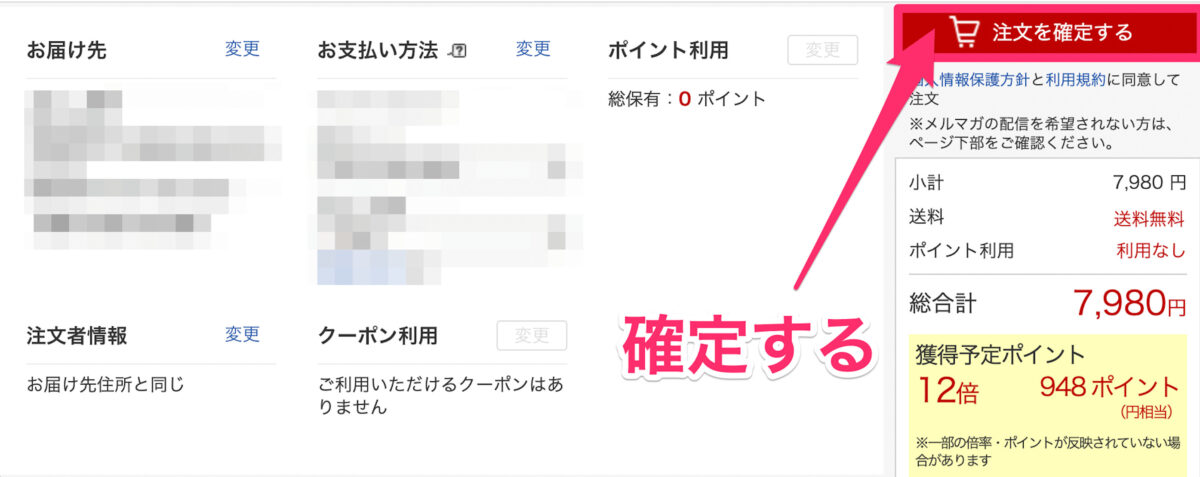
そして注文を確定して、終了だ。
 【レビュー】月の葉のCBDリキッドのフレーバー全5種を試した結果
【レビュー】月の葉のCBDリキッドのフレーバー全5種を試した結果
レビュー:月の葉のCBDリキッドのフレーバー全5種を試した結果
CBDリキッド|安いおすすめランキング5選
次に、とにかく価格が安いCBDリキッドを紹介していこう。
1位 カンナビジオール 1,320円
2位 月の葉 1,480円
3位 カンナプレッソ 1,680円
4位 HERBS 2,200円
5位 りきっど屋 3,979円
上記のとおりで、4,000円以下のリキッドもたくさんあるのだ。
安さにこだわる人は参考にしてほしい。
1位 カンナビジオール 1,320円

| 濃度 | 容量 | 種類 | 価格 |
| 0.7% | 5ml | 単一 | 1,320円 |
カンナビジオールが、今あるCBDリキッドの中で最も安いものだろう。
ただ濃度は0.7%とかなり低いため、「お試し品」として使うべきだと感じる。
2位 月の葉 1,480円
| 濃度 | 容量 | 種類 | 価格 |
| 1% | 10ml | 単一 | 1,480円 |
月の葉も、非常に安いCBDリキッドだ。
濃度は1%だが、とりあえずCBDの様子見をしたい方にはおすすめだろう。
3位 カンナプレッソ 1,680円

| 濃度 | 容量 | 種類 | 価格 |
| 1ml | 10ml | 単一 | 1,680円 |
カンナプレッソも、1%のリキッドだ。
しかしフレーバーは8種と豊富であり、選べる幅が広いことが魅力である。
・マンゴー
・メンソール
・ストロベリー
・チェリー・ミント
・フレーバーレス
・ナチュラル・ヘンプ
・ストロー・メロン・アイス
・グレープ・ブラックカラント
上記のとおりで、味わいを求める人には大きなポイントになるはずだ。
4位 HERBS 2,200円
| 濃度 | 容量 | 種類 | 価格 |
| 1% | 15ml | 単一 | 2,200円 |
総合ランキングにもランクインした、HERBSだ。
1%タイプの中での価格は高いが、日本産なため「安心感」は大きい。
質にこだわっている印象も強く受けたので、見る価値はあるだろう。
5位 りきっど屋 3,979円
| 濃度 | 容量 | 種類 | 価格 |
| 3.3% | 30ml | 単一 | 3,979円 |
| 10% | 10ml | 単一 | 3,979円 |
おすすめ8位でも紹介したリキッドだ。
上記の2タイプがあるため、自分に合ったCBDを選べるのが強み。
繰り返しになるが、フレーバーがかなり美味しかったという印象がある。
そのため、フレーバーを楽しみたい人にはこの低価格リキッドがおすすめだ。
・もも極
・メロン極
・みかん極
・メンソール
・青りんご極
・マスカット極
上記のとおり、フルーツフレーバーが多い。
やはり選びやすさが、「りきっどや」の強みだろう。
余談:安いリキッドはあまりおすすめできない
申し訳ない。
私の本音として、安いリキッドはおすすめできない。
なぜなら価格だけを見て、1%などの「うすいリキッド」を使っても、CBD感をほぼ感じれないからだ。
つまり安いリキッドを買う人は、その辺りの心づもりをしておいた方がいいだろう。
なお下手に失敗したくない人は、総合ランキングで紹介したリキッドを選んでおくのが無難だ。あちらに、ハズレはない。
高濃度リキッドのおすすめランキング
つづいて、高濃度に的を絞ったリキッドを3つ紹介しよう。
1位 プラスウィード 60%
2位 アステカ 20%
3位 ハーブス 10%
1位 +WEED(プラスウィード) 60%

| 濃度 | 容量 | 種類 | 価格 |
| 60% | 10ml | フルスペ | 73,590円 |
やはり、高濃度ならプラスウィードの一択だろう。
CBD以外にもCBG・CBDV・THCVの3種を含んだフルスペクトラム製品であり、その強烈さは最高クラスだ。
なお60%は価格も「73,590円」という最強クラスになるが、、頂点を味わいたい方にはおすすめ。国内ではTOPのリキッドになるため、買う価値は十分にあるリキッドだ。
また国産メーカーのため、「コールセンター」のお問い合わせ機能も充実している。安心感もプラスウィードの強みだろう。
2位 AZTEC(アステカ) 20%

| 濃度 | 容量 | 種類 | 価格 |
| 20% | 10ml | フルスペ | 24,800円 |
アステカも、高濃度を代表するブランドだ。
イギリス生まれの高品質なCBDを採用しており、「アステカじゃないとダメだ!」と感じるファンは私含めとても多いと思う。
1位のプラスウィードに比べると価格もリーズナブルで、海外でも人気を獲得しているCBD界の大御所だ。

このドロッとしたリキッドは本当にたまらない。1位の「73,590円」はさすがにキツすぎる・・と思った方は、ぜひこちらを検討してみてほしい。
3位 HERBS(ハーブス) 10%

| 濃度 | 容量 | 種類 | 価格 |
| 10% | 15ml | 単一 | 13,200円 |
ハーブスも、高濃度リキッドとして有名だ。
CBD先進国のアメリカから直輸入したヘンプを使用しており、吸いごたえは魅力的だった。
なお余談だが、この記事では「アステカ・ハーブス・プラスウィード・りきっどや」の4種の10%リキッドを紹介した。そしてCBD感が1番強いと感じたのは、フルスペクトラム製品であるアステカだ。
結論としてフルスペクトラム型を抜いた、つまり単一CBD製品の中では、ハーブスが最強種になるということだ。
CBDリキッドを購入する前に知っておきたいこと
最後に、予備知識を解説する。
購入する前に知っておくべきことなので、ぜひ参考にしてほしい。
その①:CBDリキッドは”やばい”?
そんなことは、一切ない。
というのも違法性もなければ、危険性もないからだ。
実際、私の知り合い3人もCBDを1年以上使っているが、CBDによって体調をくずした・・という経験はないため、その点は安心してほしい。
とはいえ、その辺りに不安があるなら、まずは下記の2記事に目を通すべきだ。
>>【合法】CBDに違法性がない理由を解説【CBD歴1年が論破する】
>>【体験記】CBDの危険性と副作用について考察【心配性な方に捧ぐ】
その②:CBDリキッドの正しい使い方とは?
ここは画像で説明しよう。

リキッドのふたには基本、「チャイルドロック」が付いている。
そのため、下に押し込みながら開けよう。
アトマイザーの”ふち”にリキッドを注いでいこう。
なお「中央の穴」は蒸気が通る道のため、ここに入れないように注意しておく必要がある。

後はバッテリーにつけて、吸うだけだ。
非常に簡単である。
以上が、リキッドの使い方だ。
その③:CBDリキッドに必要な道具とは?
リキッドを使用するには、別売りのバッテリーとアトマイザーが必要となる。
とはいえ、下記の2点を同時に購入すればOKだ。
この2点が1番安いセットになる。
私も使用しており、非常にコンパクトで使いやすい。
その④:CBDリキッドはキマる?
ネットを見ていると、「このリキッドはキマります!」といった記述を見かけることが多い。
だがしかしCBDは怪しい薬ではないため、「キマる」ことはまずありえない。おそらく、CBD感が強いことを表現していると思うのだが、この表現はふさわしくないだろう。
なので、「キマる」という言葉を見かけても不安になる必要は一切ない。CBDは自然由来の成分であり、体に害があるものではないのだ。
その⑤:何パフくらいで満足できる?
これは人それぞれによるが、私は「5~10パフ」ほどで毎日満足できている。
(※1吸いすることを、パフと呼ぶ。)
とはいえ、ここは使う濃度にもよる。私の経験上だと、下記のとおりだ。
1%〜5%→20~30パフ
10%~20%→5~10パフ
60%→3パフほど
上記のとおり、高濃度になればなるほど、少ない回数で満足できる形だ。
これは言い換えると、高濃度ほど長持ちしやすいということ。なのでコスパ良く1~2ヶ月単位で使用したい方は、10%以上のリキッドを採用すると良いだろう。
私も、基本は10%以上のリキッドしか使用しない。
その⑥:リキッドはどこで購入するのがお得なのか?
CBDMANiAだ。
記事中では何度か紹介したが、20%オフクーポンが使える。
楽天などでもリキッドは購入できるが、そのようなクーポンはないため、やはりCBDMANiAを利用しない手はない。
・Koi
・CBDfx
・アステカ
・ファーマヘンプ
なお上記の4商品なら、クーポンが使用できる。
ということで、クーポンの使用法についても解説しておこう。
まず商品ページに移動し、フレーバーとカラーを選択する。
そして、「カートに入れる」をクリックしよう。
購入する商品が正しいことを確認する。
そして、「購入手続きへ進む」をクリックしよう。
ここで、「CBDMANiA20」を入力する。
入力すれば、20%引きが適用される仕組みだ。
まず20%引きを確認しよう。そして、支払い方法の選択へと進んでいく。
なお、支払いには下記4種類が使用可能だ。
・銀行振り込み
・クレジットカード
・楽天Pay
・PayPay
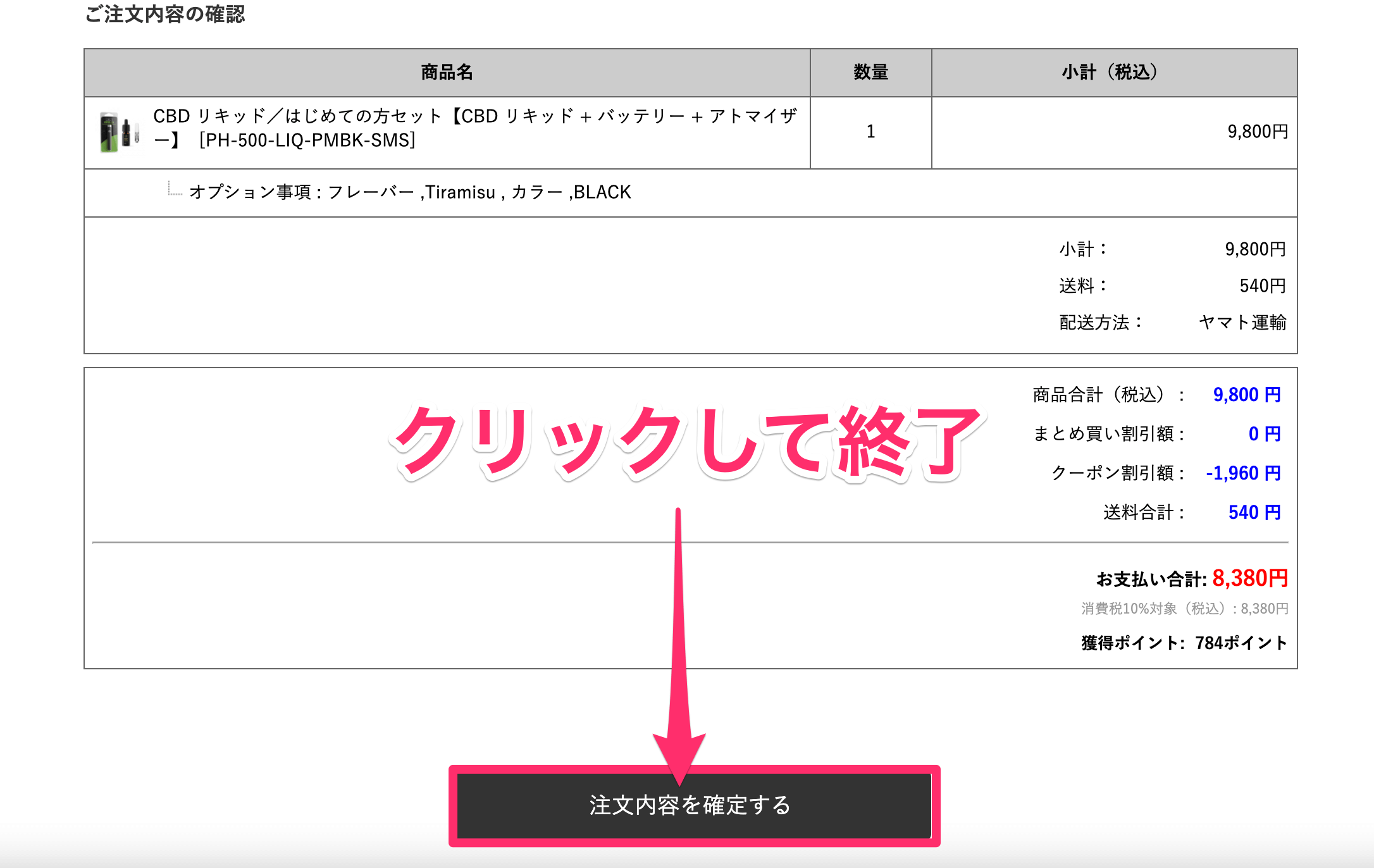
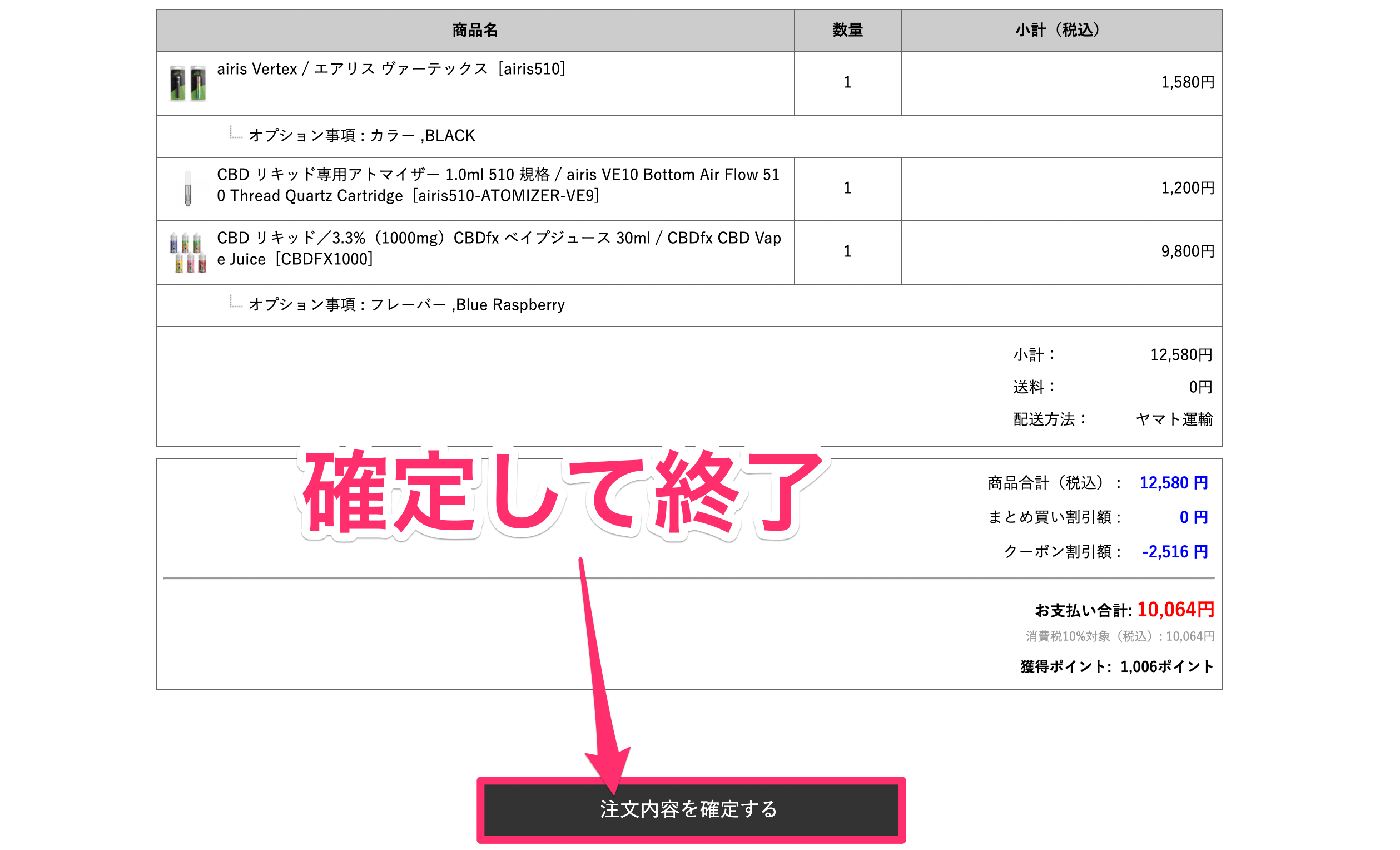
最終確認のあと、「注文内容を確定する」をクリックして終了だ。
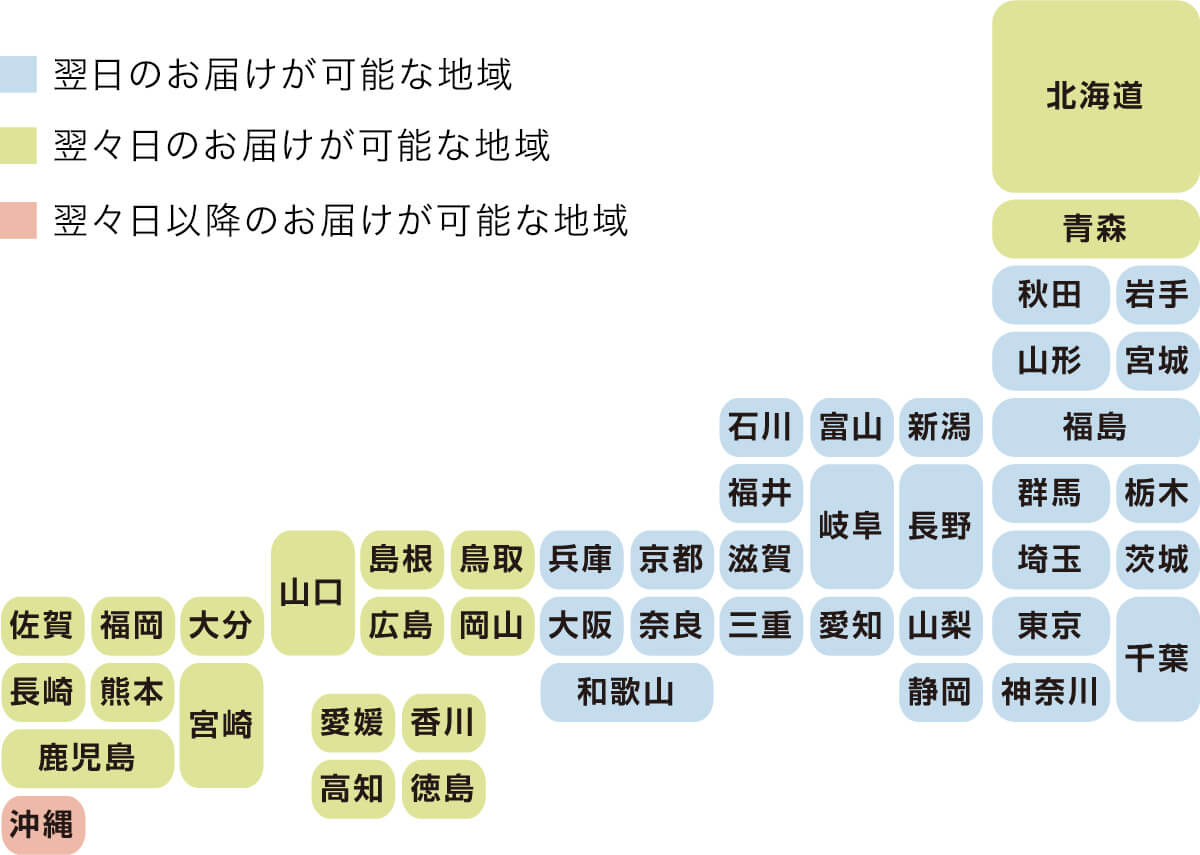
なお配送は「ヤマト運輸」のため1~2日で届く。
上記のステップをこなすだけで、20%引きとなる。
CBDは正直安くはないため、「安く買える技」も身につけておいた方が良いと思う。
ということで、おすすめランキングを再掲しておこう。
安く手に入れ、コスパ良くCBDを楽しもう。
まとめ:CBDリキッド選びに悩むならこの3品がおすすめ
結論として、初めてのCBDリキッドには、下記3つのどれかがおすすめだ。
それぞれを一言で表すと、次のとおり。
自分がどのタイプを求めるか・・という点を考えた上で、この3品から選んでほしい。
自分で言うのはおこがましいが、この3品は決して後悔はしないリキッドだと自信を持って伝えられる。
なお個人的には、ファーマヘンプが安定の1位だ。
とはいえすべてレビュー記事も書いたため、ぜひ自分に合う最高の一品を探してほしい。
それでは、今回は以上だ。